
Chapter 10: Middle Adulthood
 Objectives
Objectives
At the end of this chapter, you will be able to…
- Explain trends in life expectancy and healthy life expectancy.
- List developmental tasks of midlife.
- Summarize physical changes and health concerns that occur in midlife.
- Describe physical changes that occur during menopause and the variations in cultural responses to menopause.
- Contrast menopause and andropause.
- Explain the relationships between the climacteric and sexual expression.
- Discuss the impact of diet and exercise on health in midlife.
- Describe cognitive development in midlife including differences in crystallized and fluid intelligence.
- Contrast the expert and the novice.
- Evaluate the notion of the midlife crisis.
- Define kin-keeping and the impact of caregiving.
- Describe Erikson’s stage of generativity vs. stagnation.
- Describe personality changes in midlife.
- Discuss communication in marriage.
- Describe the stations of divorce.
- Discuss issues related to recoupling including remarriage and cohabitation.
- Describe grandparenting styles.
- Discuss work-related issues in midlife
The objectives are indicated in the reading sections below.
Middle Adulthood (Ob 1)
Middle adulthood (or midlife) refers to the period of the lifespan between young adulthood and old age. This is a relatively new period of life. One hundred years ago, life expectancy in the United States was about 47 years. This period lasts from 20 to 40 years depending on how these stages, ages, and tasks are culturally defined. The most common age definition is from 40 to 65, but there can be a range of up to 10 years on either side of these numbers. For the purpose of this text and this chapter, we will define middle adulthood from age 40 to 65. Research on this period of life is relatively new and many aspects of midlife are still being explored. This may be the least studied period of the lifespan.
Midlife as a central, pivotal period in the life course. It falls at a critical juncture examining changes that go on physically, cognitively, and socially. Midlife has a somewhat unique advantage in the life course with the juxtaposition of gains and losses for aspects of physical, cognitive, and psychosocial changes that go on. We will identify social benefits and complexities in middle adulthood in addition to identifying aspects of decline in cognitive and physical functions. And this is a varied group. We can see considerable differences in individuals within this developmental stage. There is much to learn about this group.
Developmental Tasks (Ob 2)
Lachman (2004) provides a comprehensive overview of the challenges facing midlife adults. These include:
- Losing parents and experiencing associated grief.
- Launching children into their own lives.
- Adjusting to home life without children (often referred to as the empty nest).
- Dealing with adult children who return to live at home (known as boomerang children in the United States).
- Becoming grandparents.
- Preparing for late adulthood.
- Acting as caregivers for aging parents or spouses.

We will explore these tasks and this stage of life further in this chapter.
Physical Development in Midlife (Ob 3)
There are few biologically based physical changes in midlife other than changes in vision, more joint pain, and weight gain (Lachman, 2004).
Hair: When asked to imagine someone in middle adulthood, we often picture someone with the beginnings of wrinkles and gray or thinning hair. What accounts for these physical changes? Hair color is due to a pigment called melanin which is produced by hair follicles (Martin, 2014). With aging, the hair follicles produce less melanin and this causes the hair to become gray. Hair color typically starts turning lighter at the temples, but eventually, all the hair will become white. For many, graying begins in the 30s, but it is largely determined by your genes. Gray hair occurs earlier in white people and later in Asians. Genes also determine how much hair remains on your head. Almost everyone has some hair loss with aging, and the rate of hair growth slows with aging. Many hair follicles stop producing new hairs and hair strands become smaller. Men begin showing signs of balding by 30 and some are nearly bald by 60. Male-pattern baldness is related to testosterone and is identified by a receding hairline followed by hair loss at the top of the head. Women can also develop female patterned baldness as their hair becomes less dense and the scalp becomes visible (Martin, 2014). Sudden hair loss, however, can be a symptom of a health problem.
Skin: Skin continues to dry out and is prone to more wrinkling, particularly on the sensitive face area. Wrinkles, or creases in the skin, are a normal part of aging. As we get older, our skin dries and loses the underlying layer of fat, so our face no longer appears smooth. Loss of muscle tone and thinning skin can make the face appear flabby or drooping. Although wrinkles are a natural part of aging and genetics plays a role, frequent sun exposure and smoking will cause wrinkles to appear sooner. Dark spots and blotchy skin also occur as one ages and are due to exposure to sunlight (Moskowitz, 2014). Blood vessels become more apparent as the skin continues to dry and get thinner.
Lungs: The lungs serve two functions: Supply oxygen and remove carbon dioxide. Thinning of the bones with age can change the shape of the rib cage and result in a loss of lung expansion. Age-related changes in muscles, such as the weakening of the diaphragm, can also reduce lung capacity. Both of these changes will lower oxygen levels in the blood and increase the levels of carbon dioxide. Experiencing shortness of breath and feeling tired can result (NIH, 2014b). In middle adulthood, these changes and their effects are often minimal, especially in people who are non-smokers and physically active. However, in those with chronic bronchitis, or who have experienced frequent pneumonia, asthma other lung-related disorders, or who are smokers, the effects of these normal age changes can be more pronounced.
Vision: Vision is affected by age. As we age, the lens of the eye gets larger, but the eye loses some of the flexibility required to adjust to visual stimuli. Middle-aged adults often have trouble seeing up close as a result. A typical change of the eye due to age is presbyopia, which is Latin for “old vision.” It refers to a loss of elasticity in the lens of the eye that makes it harder for the eye to focus on objects that are closer to the person. When we look at something far away, the lens flattens out; when looking at nearby objects, tiny muscle fibers around the lens enable the eye to bend the lens. With age, these muscles weaken and can no longer accommodate the lens to focus the light. Anyone over the age of 35 is at risk for developing presbyopia.
According to the National Eye Institute (NEI) (2016), signs that someone may have presbyopia include:
- Hard time reading small print
- Having to hold reading material farther than arm’s distance
- Problems seeing objects that are close
- Headaches
- Eyestrain
Another common eye problem people experience as they age are floaters, little spots or “cobwebs” that float around the field of vision. They are most noticeable if you are looking at the sky on a sunny day, or at a lighted blank screen. Floaters occur when the vitreous, a gel-like substance in the interior of the eye, slowly shrinks. As it shrinks, it becomes somewhat stringy, and these strands can cast tiny shadows on the retina. In most cases, floaters are harmless, more of an annoyance than a sign of eye problems. However, floaters that appear suddenly, or that darken and obscure vision can be a sign of more serious eye problems, such a retinal tearing, infection, or inflammation. People who are very nearsighted (myopic), have diabetes, or who have had cataract surgery are also more likely to have floaters (NEI, 2009).
During midlife, adults may begin to notice a drop in scotopic sensitivity, the ability to see in dimmer light. By age 60, the retina receives only one-third as much light as it did at age 20, making working in dimmer light more difficult (Jackson & Owsley, 2000). Night vision is also affected as the pupil loses some of its ability to open and close to accommodate drastic changes in light. Eyes become more sensitive to glare from headlights and street lights making it difficult to see people and cars, and movements outside of our direct line of sight (NIH, 2016c).
Hearing: Prior to age 40, about 5.5% of adults report hearing problems. This jumps to 19% among 40 to 69 year-olds (American Psychological Association, 2016). Hearing loss is experienced by about 14 percent of midlife adults (Gratton & Vasquez in Berk, 2007) as a result of being exposed to high levels of noise. Men may experience some hearing loss by 30 and women by 50. High-frequency sounds are the first affected by such hearing loss. This loss accumulates after years of being exposed to intense noise levels. Men are more likely to work in noisy occupations. Hearing loss is also exacerbated by cigarette smoking, high blood pressure, and stroke. Most hearing loss could be prevented by guarding against being exposed to extremely noisy environments. (There is new concern over hearing loss in early adulthood with the widespread use of earbuds)
Taking care of health
Most of the changes that occur in midlife can be easily compensated for (e.g., by buying glasses, exercising, and watching what one eats). Things like eating calcium-rich foods, such as dairy products, almonds, dark leafy greens, salmon, and tofu. Vitamin D helps the body to absorb the calcium in these foods, starting in early adulthod, can strengthen bones and teeth. Additionally, vitamin D is produced naturally by the body but can also be supplemented by foods rich in vitamin D, such as fish, eggs, mushrooms, and vitamin D–fortified foods, such as milk and cereal. Strength training also helps support balance, metabolism, and cognition (Mayo Clinic, 2023).
Hearing aids offer significant benefits for individuals with hearing loss, yet multiple studies and national surveys indicate that only about 14–29% of older adults with hearing loss in the United States use hearing aids, with usage rates increasing with age and severity of hearing loss. Supportive health care for hearing loss is essential as untreated hearing loss can hinder work, social interactions, daily activities, and even lead to stress, fatigue, and impaired brain function. Preventative care is important, and most midlife adults experience general good health. However, the percentage of adults who have a disability increases through midlife; while 7 percent of people in their early 40s have a disability, the rate jumps to 30 percent by the early 60s. This increase is highest among those of lower socioeconomic status (Bumpass & Aquilino, 1995).
Midlife adults have to increase their level of exercise, eat less, and watch their nutrition to maintain their earlier physique. However, weight can can happen due to decreased metabolism. Sometimes referred to as the middle-aged spread, the accumulation of fat in the abdomen, is one of the common complaints of midlife adults. Men tend to gain fat on their upper abdomen and back while women tend to gain more fat on their waist and upper arms. Many adults are surprised at this weight gain because their diets have not changed. However, the metabolism slows during midlife by about one-third (Berger, 2005). Recently semaglutide hormone therapies are being used as medical approaches to weight management, particularly for adults at risk for diabetes and cardiovascular disease. Semaglutide acts on the hypothalamus to reduce appetite and food intake, and initial studies have found promising results for patients using these injectable medications to sustain weight loss and lower risk of cardiovascular disease and diabetes (Lincoff et al., 2023). Semaglutide, a GLP-1 receptor agonist originally developed for type 2 diabetes, is now FDA-approved as Wegovy for weight management and works by reducing appetite and food intake, with studies showing it helps sustain weight loss and lower cardiovascular and diabetes risk, though more research is needed on its long-term safety and effectiveness.
It becomes important for midlife adults to take preventative measures to enhance physical well-being. Again, lifestyle has a strong impact on the health status of midlife adults. Choosing not to smoke, watch intake of alcohol, have a good diet, reduce stress and keep up on physical activity can improve overall health. Those midlife adults who have a strong sense of mastery and control over their lives, who engage in challenging physical and mental activity, who engage in weight bearing exercise, monitor their nutrition, and make use of social resources are most likely to enjoy a plateau of good health through these years (Lachman, 2004).
Health Concerns
Sarcopenia: The loss of muscle mass and strength that occurs with aging is referred to as Sarcopenia (Morley et al., 2001). Sarcopenia is thought to be a significant factor in the frailty and functional impairment that occurs when older. The decline of growth and anabolic hormones, especially testosterone, and decreased physical activity have been implicated as causes of sarcopenia (Proctor et al., 1998). This decline in muscle mass can occur as early as 40 years of age and contributes significantly to a decrease in life quality, increase in health care costs, and early death in older adults (Karakelides & Nair, 2005). In middle age, muscular performance gradually declines at a rate of approximately five percent every ten years. While men and women generally experience a loss of 30 to 40 percent of their functional strength, people can counteract the loss of muscle mass in later years by engaging in a strength training regimen. Sarcopenia has only recently been recognized an independent disease entity since 2016 (ICD-10). In 2018 the U.S. Center for Disease Control and prevention assigned sarcopenia its own discrete medical code. Exercise is certainly important to increase strength, aerobic capacity, muscle protein synthesis, and new nerve growth (Piasescki et al, 2018), but unfortunately, it does not reverse all the age-related changes that occur. The muscle-to-fat ratio for both men and women also changes throughout middle adulthood, with an accumulation of fat in the stomach area. Human beings reach peak bone mass around 35-40. Mobility can central concern, and some researchers are now identifying some conditions like osteosarcopenia, which describes the decline of both muscle tissue (sarcopenia) and bone tissue (osteoporosis).
Heart Disease: According to the most recent National Vital Statistics Reports (Xu et al., 2016) heart disease continues to be the number one cause of death for Americans as it claimed 23.5% of those who died in 2013. It is also the number one cause of death worldwide (WHO, 2019). Heart disease develops slowly over time and typically appears in midlife (Hooker & Pressman, 2016). Heart disease can include heart defects and heart rhythm problems, as well as narrowed, blocked, or stiffened blood vessels referred to as a cardiovascular disease. The blocked blood vessels prevent the body and heart from receiving adequate blood. Atherosclerosis, or a buildup of fatty plaque in the arteries, is the most common cause of cardiovascular disease. The plaque buildup thickens the artery walls and restricts the blood flow to organs and tissues. Cardiovascular disease can lead to a heart attack, chest pain (angina), or stroke (Mayo Clinic, 2014a).
Complications of heart disease can include heart failure when the heart cannot pump enough blood to the meet the body’s needs, and a heart attack, when a blood clot blocks the blood flow to the heart. This blockage can damage or destroy a part of the heart muscle, and atherosclerosis is a factor in a heart attack. Treatment for heart disease includes medication, surgery, and lifestyle changes including exercise, healthy diet, and refraining from smoking.
Sudden cardiac arrest is the unexpected loss of heart functioning, breathing, and consciousness, often caused by an arrhythmia or abnormal heartbeat. The heartbeat may be too quick, too slow, or irregular. With a healthy heart, it is unlikely for a fatal arrhythmia to develop without an outside factor, such as an electric shock or illegal drugs. If not treated immediately, sudden cardiac arrest can be fatal and result in sudden cardiac death.
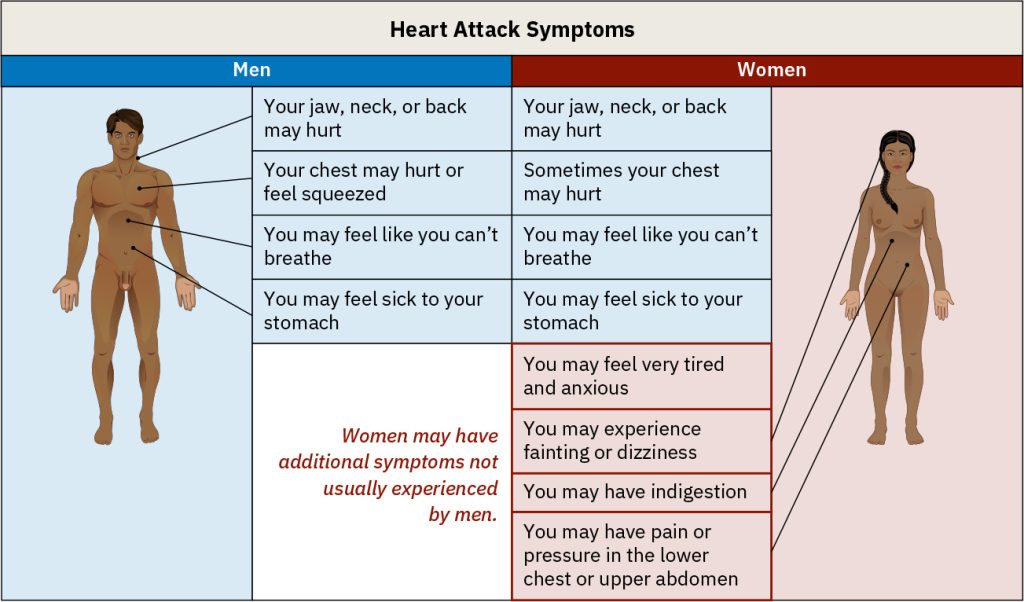
Symptoms of cardiovascular diseases (including heart disease) differ for men and women. Males are more likely to suffer chest pain. Symptoms may include acute [chest] pain, weakness, dizziness, confusion, and shortness of breath. In fact, chest pain, such as pressure, squeezing, or fullness is a major indicator that doctors look for when diagnosing a heart attack (Becker, 2005). However, women are more likely to demonstrate shortness of breath, nausea, and extreme fatigue. The three most common early warning symptoms among women are extreme fatigue, trouble sleeping, and shortness of breath (even when not engaging in physical exertion). Other symptoms can also include pain in the arms, legs, neck, jaw, throat, abdomen, or back (Mayo Clinic, 2014a). It is important for women and their loved ones to be aware of these symptoms and get medical attention immediately in an acute situation. The most common acute symptoms include shortness of breath, weakness, and fatigue. In addition, prevention and early intervention are also important. A diet low in trans and saturated fat, no smoking, and regular exercise and stress reduction are good preventative measures.
Hypertension, or high blood pressure, is a serious health problem that occurs when the blood flows with a greater force than normal. One in three American adults (70 million people) have hypertension and only half have it under control (Nwankwo, Yoon, Burt, & Gu, 2013). It can strain the heart, increase the risk of heart attack and stroke, or damage the kidneys (CDC, 2014a). Uncontrolled high blood pressure in early and middle adulthood can also damage the brain’s white matter (axons) and may be linked to cognitive problems later in life (Maillard et al., 2012). Normal blood pressure is under 120/80. The first number is the systolic pressure, which is the pressure in the blood vessels when the heart beats. The second number is the diastolic pressure, which is the pressure in the blood vessels when the heart is at rest. High blood pressure is sometimes referred to as the silent killer, as most people with hypertension experience no symptoms.
High Cholesterol: Cholesterol is a waxy fatty substance carried by lipoprotein molecules in the blood. It is created by the body to create hormones and digest fatty foods and is also found in many foods. Your body needs cholesterol, but too much can cause heart disease and stroke. Two important kinds of cholesterol are low-density lipoprotein (LDL) and high-density lipoprotein (HDL). The third type of fat is called triglycerides. Your total cholesterol score is based on all three types of lipids. LDL cholesterol makes up the majority of the body’s cholesterol, however, it is often referred to as “bad” cholesterol because at high levels it can form plaque in the arteries leading to heart attack and stroke. HDL cholesterol often referred to as “good” cholesterol, absorbs cholesterol, and carries it back to the liver, where it is then flushed from the body. Higher levels of HDL can reduce the risk of heart attack and stroke. Triglycerides are a type of fat in the blood used for energy. High levels of triglycerides can also increase your risk for heart disease and stroke when coupled with high LDL and low HDL. All adults 20 or older should have their cholesterol checked. In early adulthood, doctors may check every few years if the numbers have previously been normal, and there are no other signs of heart disease. In middle adulthood, this may become part of the annual check-up (CDC, 2015).
Cancer: After heart disease, cancer was the second leading cause of death for Americans in 2013 as it accounted for 22.5% of all deaths (Xu et al., 2016). According to the National Institutes of Health (2015), cancer is the name given to a collection of related diseases in which the body’s cells begin to divide without stopping and spread into surrounding tissues. These extra cells can divide and form growths called tumors, which are typically masses of tissue. Cancerous tumors are malignant, which means they can invade nearby tissues. When removed malignant tumors may grow back. Unlike malignant tumors, benign tumors do not invade nearby tissues. Benign tumors can sometimes be quite large, and when removed usually do not grow back. Although benign tumors in the body are not cancerous, benign brain tumors can be life-threatening. Cancer cells can prompt nearby normal cells to form blood vessels that supply the tumors with oxygen and nutrients, which allows them to grow. These blood vessels also remove waste products from the tumors. Cancer cells can also hide from the immune system, a network of organs, tissues, and specialized cells that protects the body from infections and other conditions. Lastly, cancer cells can metastasize, which means they can break from where they first formed, called primary cancer, and travel through the lymph system or blood to form new tumors in other parts of the body. This new metastatic tumor is the same type as the primary tumor (National Institutes of Health, 2015).
Cancer can start almost anywhere in the human body. While normal cells mature into very distinct cell types with specific functions, cancer cells do not and continue to divide without stopping. Further, cancer cells are able to ignore the signals that normally tell cells to stop dividing or to begin a process known as programmed cell death which the body uses to get rid of unneeded cells. With the growth of cancer cells, normal cells are crowded out and the body is unable to work the way it is supposed to. For example, the cancer cells in lung cancer form tumors which interfere with the functioning of the lungs and how oxygen is transported to the rest of the body. There are more than 100 types of cancer. The American Cancer Society assemblies a list of the most common types of cancers in the United States. To qualify for the 2016 list, the estimated annual incidence had to be 40,000 cases or more. The most common type of cancer on the list is breast cancer. The next most common cancers are lung cancer and prostate cancer (American Cancer Society, 2016).
Diabetes (Diabetes Mellitus) is a disease in which the body does not control the amount of glucose in the blood. A typical test for diabetes includes a fasting glucose test. This disease occurs when the body does not make enough insulin or does not use it the way it should (NIH, 2016a). Insulin is a type of hormone that helps glucose in the blood enter cells to give them energy. In adults, 90% to 95% of all diagnosed cases of diabetes are type 2 (American Diabetes Association, 2016). Type 2 diabetes usually begins with insulin resistance, a disorder in which the cells in the muscles, liver, and fat tissue do not use insulin properly (CDC, 2014d). As the need for insulin increases, cells in the pancreas gradually lose the ability to produce enough insulin. In some Type 2 diabetics, pancreatic beta cells will cease functioning, and the need for insulin injections will become necessary. Some people with diabetes experience insulin resistance with only minor dysfunction of the beta cell secretion of insulin. Other diabetics experience only slight insulin resistance, with the primary cause being a lack of insulin secretion (CDC, 2014d). One in three adults are estimated to have prediabetes, and 9 in 10 of them do not know. According to the CDC (2014d) without intervention, 15% to 30% of those with prediabetes will develop diabetes within 5 years. In 2012, 29 million people (over 9% of the population) were living with diabetes in America, most adults age 20 and up. The median age of diagnosis is 54 (CDC, 2014d). During middle adulthood, the number of people with diabetes dramatically increases; with 4.3 million living with diabetes prior to age 45, to over 13 million between the ages of 45 to 64; a four-fold increase. Men are slightly more likely to experience diabetes than are women.
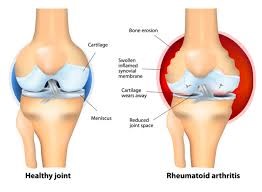
Rheumatoid arthritis (RA) is an inflammatory disease that causes pain, swelling, stiffness, and loss of function in the joints (NIH, 2016b). Between 30 and 60 is the typical onset age for rheumatoid arthritis (RA), with the peak onset for women being sometime in the early 40s. RA occurs when the immune system attacks the membrane lining the joints. RA is the second most common form of arthritis after osteoarthritis, which is the normal wear and tear the joints. Unlike osteoarthritis, RA is symmetric in its attack of the body, thus, if one shoulder is affected so is the other. In addition, those with RA may experience fatigue and fever.
Common features of RA (NIH, 2016b):
- Tender, warm, swollen joints
- Symmetrical pattern of affected joints
- Joint inflammation often affecting the wrist and finger joints closest to the hand
- Joint inflammation sometimes affecting other joints, including the neck, shoulders, elbows, hips, knees, ankles, and feet
- Fatigue, occasional fevers, a loss of energy
- Pain and stiffness lasting for more than 30 minutes in the morning or after a long rest
- Symptoms that last for many years
About 1.5 million people (approximately 0.6%) of Americans experience rheumatoid arthritis. It occurs across all races and age groups, although the disease often begins in middle adulthood and occurs with increased frequency in older people. Like some other forms of arthritis, rheumatoid arthritis occurs much more frequently in women than in men. About two to three times as many women as men have the disease (NIH, 2016b). It affects women more than men by a factor of around 3 to 1. The lifetime risk for RA for women is 3.6% and 1.7% for men (Crowson et al., 2011).
Genes play a role in the development of RA. However, individual genes by themselves confer only a small risk of developing the disease, as some people who have these particular genes never develop RA. Scientists think that something must occur to trigger the disease process in people whose genetic makeup makes them susceptible to rheumatoid arthritis. For instance, some scientists also think hormonal factors may be involved. In women who experience RA, the symptoms may improve during pregnancy and flare after pregnancy. Women who use oral contraceptives may increase their likelihood of developing RA. This suggests hormones, or possibly deficiencies or changes in certain hormones may increase the risk of developing RA in a genetically susceptible person (NIH, 2016b).
Rheumatoid arthritis can affect virtually every area of a person’s life, and it can interfere with the joys and responsibilities of work and family life. Fortunately, current treatment strategies allow most people with RA to lead active and productive lives. Pain-relieving drugs and medications can slow joint damage, and establishing a balance between rest and exercise can also lessen the symptoms of RA (NIH, 2016b).
Digestive Issues
In the U.S. 60 million people experience heartburn at least once a month, and 15 million experience it every day. Heartburn, also called acid indigestion or pyrosis, is a common digestive problem in adults and is the result of stomach acid backing up into the esophagus. Prolonged contact with the digestive juices injures the lining of the esophagus and causes discomfort. Heartburn that occurs more frequently may be due to gastroesophageal reflux disease, GERD. Normally the lower sphincter muscle in the esophagus keeps the acid in the stomach from entering the esophagus. In GERD this muscle relaxes too frequently and the stomach acid flows into the esophagus. Prolonged problems with heartburn can lead to more serious complications, including esophageal cancer, one of the most lethal forms of cancer in the U.S. Problems with heartburn can be linked to eating fatty or spicy foods, caffeine, smoking, and eating before bedtime (American College of Gastroenterology, 2016a).
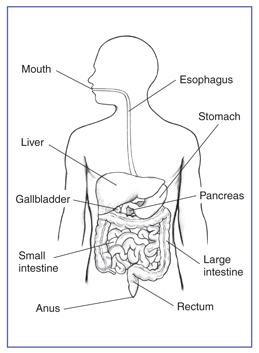 Gallstones are present in about 20% of women and 10% of men over the age of 55 (American College of Gastroenterology, 2016b). Gallstones are hard particles, including fatty materials, bile pigments, and calcium deposits, that can develop in the gallbladder. Ranging in size from a grain of sand to a golf ball, they typically take years to develop, but in some people have developed over the course of a few months. About 75% of gallstones do not create any symptoms, but those that do may cause sporadic upper abdominal pain when stones block bile or pancreatic ducts. If stones become lodged in the ducts, it may necessitate surgery or other medical intervention as it could become life-threatening if left untreated (American College of Gastroenterology, 2016b). Risk factors for gallstones include a family history of gallstones, diets high in calories and refined carbohydrates (such as, white bread and rice), diabetes, metabolic syndrome, Crohn’s disease, and obesity, which increases the cholesterol in the bile and thus increases the risk of developing gallstones (NIH, 2013).
Gallstones are present in about 20% of women and 10% of men over the age of 55 (American College of Gastroenterology, 2016b). Gallstones are hard particles, including fatty materials, bile pigments, and calcium deposits, that can develop in the gallbladder. Ranging in size from a grain of sand to a golf ball, they typically take years to develop, but in some people have developed over the course of a few months. About 75% of gallstones do not create any symptoms, but those that do may cause sporadic upper abdominal pain when stones block bile or pancreatic ducts. If stones become lodged in the ducts, it may necessitate surgery or other medical intervention as it could become life-threatening if left untreated (American College of Gastroenterology, 2016b). Risk factors for gallstones include a family history of gallstones, diets high in calories and refined carbohydrates (such as, white bread and rice), diabetes, metabolic syndrome, Crohn’s disease, and obesity, which increases the cholesterol in the bile and thus increases the risk of developing gallstones (NIH, 2013).
The Climacteric (Ob 4, Ob 5, Ob 6)
One biologically based change that occurs during midlife is the climacteric. The climacteric, or the midlife transition when fertility declines, is biologically based but impacted by the environment. During midlife, men may experience a reduction in their ability to reproduce. Women, however, lose their ability to reproduce once they reach menopause.
Menopause for women: Perimenopause refers to a period of transition in which a woman’s ovaries stop releasing eggs and the level of estrogen and progesterone production decreases. Menopause is defined as 12 months without menstruation. After menopause, a woman’s menstruation ceases (U. S. National Library of Medicine and National Institute of Health, 2007).
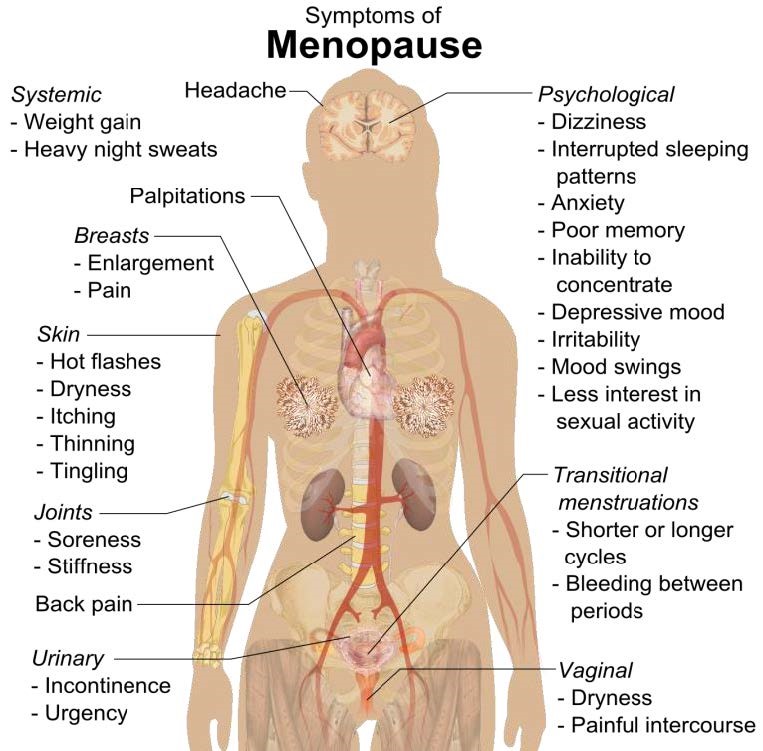
Changes typically occur between the mid-40s and mid-50s. Many women begin experiencing symptoms in their 40s. These symptoms occur during perimenopause, which can occur 2 to 8 years before menopause (Huang, 2007). A woman may first begin to notice that her periods are more or less frequent than before. These changes in menstruation may last from 1 to 3 years. After a year without menstruation, a woman is considered menopausal and no longer capable of reproduction. (Keep in mind that some women, however, may experience another period even after going for a year without one.) The median age range for women to have her last menstrual period is 50-52, but ages vary. The loss of estrogen also affects vaginal lubrication which diminishes and becomes waterier. The vaginal wall also becomes thinner, and less elastic. The shifting hormones can contribute to the inability to fall asleep. Additionally, the declining levels of estrogen may make a woman more susceptible to environmental factors and stressors which disrupt sleep. A hot flash is a surge of adrenaline that can awaken the brain from sleep. It often produces sweat and a change of temperature that can be disruptive to sleep and comfort levels. Unfortunately, it may take time for adrenaline to recede and allow sleep to occur again (National Sleep Foundation, 2016). Decreased estrogen can cause osteoporosis resulting in decreased bone mass. Depression, irritability, and weight gain are often associated with menopause, but they are not menopausal (Avis et al., 2001; Rossi, 2004). Weight gain can occur due to an increase in intra-abdominal fat followed by a loss of lean body mass after menopause (Morita et al., 2006). Consequently, women may need to change their lifestyle to counter any weight gain. Most American women go through menopause with few problems (Carroll, 2016). Overall, menopause is not seen as universally distressing (Lachman, 2004).
Hormone Replacement Therapy: Concerns about the effects of hormone replacement has changed the frequency with which estrogen replacement and hormone replacement therapies have been prescribed for menopausal women. Estrogen replacement therapy was once commonly used to treat menopausal symptoms. However, more recently, hormone replacement therapy has been associated with breast cancer, stroke, and the development of blood clots (NIH, 2007). Most women do not have symptoms severe enough to warrant estrogen or hormone replacement therapy. If so, they can be treated with lower doses of estrogen and monitored with more frequent breast and pelvic exams. There are also some other ways to reduce symptoms. These include avoiding caffeine and alcohol, eating soy, remaining sexually active, practicing relaxation techniques, and using water-based lubricants during intercourse.

Cultural influences seem to also play a role in the way menopause is experienced. Numerous international students enrolled in my class have expressed their disbelief when we discuss menopause. For example, after listing the symptoms of menopause, a woman from Kenya or Nigeria might respond, “We do not have this in my country or if we do, it is not a big deal” to which some U. S. students reply, “I want to go there!” Indeed, there are cultural variations in the experience of menopausal symptoms. Hot flashes are experienced by 75 percent of women in Western cultures, but by less than 20 percent of women in Japan (Obermeyer in Berk, 2007).
Women in the United States respond differently to menopause depending upon the expectations they have for themselves and their lives. White, career-oriented women, African-American, and Mexican-American women overall tend to think of menopause as a liberating experience. Nevertheless, there has been a popular tendency to erroneously attribute frustrations and irritations expressed by women of menopausal age to menopause and thereby not take her concerns seriously. Fortunately, many practitioners in the United States today are normalizing rather than pathologizing menopause.
Concerns about the effects of hormone replacement have changed the frequency with which estrogen replacement and hormone replacement therapies have been prescribed for menopausal women. Estrogen replacement therapy was once commonly used to treat menopausal symptoms. But more recently, hormone replacement therapy has been associated with breast cancer, stroke, and the development of blood clots (NLM/NIH, 2007). Most women do not have symptoms severe enough to warrant estrogen or hormone replacement therapy. But if so, they can be treated with lower doses of estrogen and monitored with more frequent breast and pelvic exams. There are also some other ways to reduce symptoms. These include avoiding caffeine and alcohol, eating soy, remaining sexually active, practicing relaxation techniques, and using water-based lubricants during intercourse.
Andropause for men: Do males experience a climacteric? They do not lose their ability to reproduce as they age, although they do tend to produce lower levels of testosterone and fewer sperm. Andropause is related to decreases in testosterone levels that occur with age. However, men are capable of reproduction throughout life. It is natural for sex drive to diminish slightly as men age, but a lack of sex drive may be a result of extremely low levels of testosterone. About 5 million men experience low levels of testosterone that results in symptoms such as a loss of interest in sex, loss of body hair, difficulty achieving or maintaining an erection, loss of muscle mass, and breast enlargement. Low testosterone levels may be due to glandular disease such as testicular cancer. Testosterone levels can be tested and if they are low, men can be treated with testosterone replacement therapy. This can increase sex drive, muscle mass, and beard growth. However, long term HRT for men can increase the risk of prostate cancer (The Patient Education Institute, 2005).
Although males can continue to father children throughout middle adulthood, erectile dysfunction (ED) becomes more common. Erectile dysfunction refers to the inability to achieve an erection or an inconsistent ability to achieve an erection (Swierzewski, 2015). Intermittent ED affects as many as 50% of men between the ages of 40 and 70. About 30 million men in the United States experience chronic ED, and the percentages increase with age. Approximately 4% of men in their 40s, 17% of men in their 60s, and 47% of men older than 75 experience chronic ED. Causes for ED are primarily due to medical conditions, including diabetes, kidney disease, alcoholism, and atherosclerosis (build-up of plaque in the arteries). Overall, diseases account for 70% of chronic ED, while psychological factors, such as stress, depression and anxiety account for 10%-20% of all cases. Many of these causes are treatable, and ED is not an inevitable result of aging. Men during middle adulthood may also experience prostate enlargement, which can interfere with urination, and deficient testosterone levels which decline throughout adulthood, but especially after age 50.
The Climacteric and Sexuality (Ob 7)

Sexuality is an important part of people’s lives at any age. Midlife adults tend to have sex lives that are very similar to that of younger adults. And many women feel freer and less inhibited sexually as they age. However, a woman may notice less vaginal lubrication during arousal and men may experience changes in their erections from time to time. This is particularly true for men after age 65. As discussed in the previous paragraph, men who experience consistent problems are likely to have medical conditions (such as diabetes or heart disease) that impact sexual functioning (National Institute on Aging, 2005).
Results from the National Social Life Health, and Aging Project indicated that 72% of men and 45.5% of women aged 52 to 72 reported being sexually active (Karraker et al., 2011). Couples continue to enjoy physical intimacy and may engage in more foreplay, oral sex, and other forms of sexual expression rather than focusing as much on sexual intercourse. Continued sexual activity is linked to better psychological and cognitive health—including lower depression risk and improved memory—with research suggesting a bidirectional relationship, as both good health can promote sexual activity and sexual intimacy can enhance mood, belonging, and cognitive function, possibly due to neurotransmitter release (Jackson et al, 2019; Wright & Jenks, 2016).
Risk of pregnancy continues until a woman has been without menstruation for at least 12 months, however, and couples should continue to use contraception. People continue to be at risk of contracting sexually transmitted infections such as genital herpes, chlamydia, and genital warts. In 2014, 16.7% of the country’s new HIV diagnoses (7,391 of 44,071) were among people 50 and older, according to the Centers for Disease Control and Prevention (2014e). This was an increase from 15.4% in 2005. Practicing safe sex is important at any age, but unfortunately adults over the age of 40 have the lowest rates of condom use (Center for Sexual Health Promotion, 2010). This low rate of condom use suggests the need to enhance education efforts for older individuals regarding STI risks and prevention. Hopefully, when partners understand how aging affects sexual expression, they will be less likely to misinterpret these changes as a lack of sexual interest or displeasure in the partner and more able to continue to have satisfying and safe sexual relationships.
Sleep
According to the American Academy of Sleep Medicine (Kasper, 2015), adults require at least 7 hours of sleep per night to avoid the health risks associated with chronic sleep deprivation. Less than 6 hours and more than 10 hours is also not recommended for those in middle adulthood (National Sleep Foundation, 2024). Not surprisingly, many Americans do not receive the 7-9 hours of sleep recommended. In 2013, only 59% of U.S. adults met that standard, while in 1942, 84% did (Jones, 2013). This means 41% of Americans receive less than the recommended amount of nightly sleep. Additional results included that in 1993, 67% of Americans felt they were getting enough sleep, but in 2013 only 56% felt they received as much sleep as needed. According to a 2016 National Center for Health Statistics analysis (CDC, 2016) having children decreases the amount of sleep an individual receives, however, having a partner can improve the amount of sleep for both males and females. Additionally, 43% of Americans in 2013 believed they would feel better with more sleep.
Sleep problems: According to the Sleep in America poll (National Sleep Foundation, 2015), 9% of Americans report being diagnosed with a sleep disorder, and of those 71% have sleep apnea, and 24% suffer from insomnia. Pain is also a contributing factor in the difference between the amount of sleep Americans say they need and the amount they are getting. An average of 42 minutes of sleep debt occur for those with chronic pain, and 14 minutes for those who have suffered from acute pain in the past week. Stress and overall poor health are also key components of shorter sleep duration and worse sleep quality. Those in midlife with lower life satisfaction experienced a greater delay in the onset of sleep than those with higher life satisfaction. Delayed onset of sleep could be the result of worry and anxiety during midlife, and improvements in those areas should improve sleep. Lastly, menopause can affect a woman’s sleep duration and quality (National Sleep Foundation, 2016).
Negative consequences of insufficient sleep: There are many consequences of too little sleep, and they include physical, cognitive, and emotional changes. Sleep deprivation suppresses immune responses that fight off infection and can lead to obesity, memory impairment, and hypertension (Ferrie et al., 2007; Kushida, 2005). Insufficient sleep is linked to an increased risk for colon cancer, breast cancer, heart disease, and type 2 diabetes (Pattison, 2015). A lack of sleep can increase stress as cortisol (a stress hormone) remains elevated which keeps the body in a state of alertness and hyperarousal which increases blood pressure. Sleep is also associated with longevity. Dew et al. (2003) found that older adults who had better sleep patterns also lived longer. During deep sleep, a growth hormone is released which stimulates protein synthesis, breaks down fat that supplies energy, and stimulates cell division. Consequently, a decrease in deep sleep contributes to less growth hormone being released and subsequent physical decline seen in aging (Pattison, 2015). Sleep disturbances can also impair glucose functioning in middle adulthood. Caucasian, African American, and Chinese non-shift-working women aged 48–58 years who were not taking insulin-related medications participated in the Study of Women’s Health Across the Nation (SWAN) Sleep Study and were subsequently examined approximately 5 years later (Taylor et al., 2016). Body mass index (BMI) and insulin resistance were measured at two time points. Results indicated that irregular sleep schedules, including highly variable bedtimes and staying up much later than usual, are associated in midlife women with insulin resistance, which is an important indicator of metabolic health, including diabetes risk. Diabetes risk increases in midlife women and irregular sleep schedules may be an important reason because disrupting circadian timing may impair glucose metabolism and energy homeostasis.

Stress
We all know that stress plays a major role in our mental and physical health, but what exactly is stress? The term stress is defined as a pattern of physical and psychological responses in an organism after it perceives a threatening event that disturbs its homeostasis and taxes its abilities to cope with the event (Hooker & Pressman, 2016). Stress was originally derived from the field of mechanics where it is used to describe materials under pressure. The word was first used in a psychological manner by researcher Hans Selye. Selye (1946) coined the term stressor to label a stimulus that had this effect on the body (that is, causing stress). He developed a model of the stress response called the General Adaptation Syndrome, which is a three-phase model of stress, which includes a mobilization of physiological resources phase, a coping phase, and an exhaustion phase (i.e., when an organism fails to cope with the stress adequately and depletes its resources).
Psychologists have studied stress in a myriad of ways, and it is not just major life stressor (e.g., a family death, a natural disaster) that increase the likelihood of getting sick. Stress can result from negative events, chronically difficult situations, a biological fight-or-flight response, and as clinical illness, such as post-traumatic stress disorder (PTSD). Even small daily hassles, like getting stuck in traffic or fighting with your friend, can raise your blood pressure, alter your stress hormones, and even suppress your immune system function (DeLongis et al., 1988; Twisk et al., 1999). Stress continues to be one of the most important and well-studied psychological correlates of illness because excessive stress causes potentially damaging wear and tear on the body and can influence almost any disease process.

Dispositions and Stress: Negative dispositions and personality traits have been strongly tied to an array of health risks. One of the earliest negative trait-to-health connections was discovered in the 1950s by two cardiologists. They made the interesting discovery that there were common behavioral and psychological patterns among their heart patients that were not present in other patient samples. This pattern included being competitive, impatient, hostile, and time urgent. These patterns of behavior were associated with double the risk of heart disease as compared with those who did not display those behaviors (Friedman & Rosenman, 1959). Since the 1950s, researchers have discovered that it is the hostility and competitiveness components of personality are especially harmful to heart health (Irribarren et al., 2000; Matthews et al., 1977; Miller et al., 1996). Hostile individuals are quick to get upset, and this angry arousal can damage the arteries of the heart. In addition, given their negative personality style, hostile people often lack a health-protective supportive social network.
Social Relationships and Stress: Research has shown that the impact of social isolation on our risk for disease and death is similar in magnitude to the risk associated with smoking regularly (Holt-Lunstad et al., 2010; House et al., 1988). In fact, the importance of social relationships for our health is so significant that some scientists believe our body has developed a physiological system that encourages us to seek out our relationships, especially in times of stress (Taylor et al., 2000). Social integration is the concept used to describe the number of social roles that you have (Cohen & Willis, 1985). For example, you might be a daughter, a basketball team member, a Humane Society volunteer, a coworker, or a student. Maintaining these different roles can improve your health via encouragement from those around you to maintain a healthy lifestyle. Those in your social network might also provide you with social support (e.g., when you are under stress). This support might include emotional help (e.g., a hug when you need it), tangible help (e.g., lending you money), or advice. By helping to improve health behaviors and reduce stress, social relationships can have a powerful, protective impact on health, and in some cases, might even help people with serious illnesses stay alive longer (Spiegel et al., 1989).
Social support is important to buffer stress, but caregiving and spousal care can add stress. A disabled child, spouse, parent, or other family member is part of the lives of some midlife adults. Caregiving for a young or adult child with special needs was associated with poorer global health and more physical symptoms among both fathers and mothers (Seltzer et al., 2011). Stress is felt when a caregiving spouse feels strain (Beach et al., 2000; Krause et al., 1992; Schulz et al., 1997). Women experience more caregiving burden than men, despite similar caregiving situations (Gibbons et al., 2014; Torti et al., 2004; Yeager et al., 2010). Women do not use more external support because they feel responsible to assume the caregiving roles (Torti et al, 2004) and have concerns with the opinions of others if they accepted help (Arai et al., 2000). Of concern for caregiving is that disabled males are more aggressive than females, especially males with dementia who display more physical and sexual aggression toward their caregivers (Eastley & Wilcock, 1997; Zuidema et al., 2009).
Exercise, Nutrition, Coping, and Health (Ob 8, Ob 9)

Lifestyle has a strong impact on the health status of midlife adults. Smoking tobacco, drinking alcohol, poor diet, stress, physical inactivity, and chronic diseases such as diabetes or arthritis reduce overall health. It becomes important for midlife adults to take preventative measures to enhance physical well-being. Those midlife adults who have a strong sense of mastery and control over their lives, who engage in challenging physical and mental activity, who engage in weight-bearing exercise, monitor their nutrition, and make use of social resources are most likely to enjoy a plateau of good health through these years (Lachman, 2004). This next section reviews positive ways to keep health in middle adulthood.
Exercise
The impact of exercise: Exercise is a powerful way to combat the changes we associate with aging. Exercise plays an important role in counteract normal aging. Exercise builds muscle, increases metabolism, helps control blood sugar, increases bone density, and relieves stress. Unfortunately, fewer than half of midlife adults’ exercise and only about 20 percent exercise frequently and strenuously enough to achieve health benefits. Exercise increases the levels of serotonin (Young, 2007). Physical activity is also related to reductions in depression and anxiety (De Moor et al., 2006). For example, individuals who regularly exercise are less depressed or anxious than those who do not (De Moor et al., 2006). The health benefits that walking and other physical activity have on the nervous system are becoming increasingly obvious to those who study aging. Adami et al (2018) found pronounced links between weight-bearing exercise and neuron production. Many studies suggest that voluntary physical activity extends and improves quality of life. Such studies show that even moderate physical activity can bring large gains. Exercise tends to reduce and prevent behaviors such as smoking, alcohol, and gambling, and to regulate the impulse for hunger and satiety (Vatansever-Ozen et al., 2011; Tiryaki-Sonmez et al., 2015).
The best exercise programs are those that are engaged in regularly-regardless of the activity. But a well-rounded program that is easy to follow includes walking and weight training. Having a safe, enjoyable place to walk can make a difference in whether or not someone walks regularly. Weight lifting and stretching exercises at home can also be part of an effective program. Exercise is particularly helpful in reducing stress in midlife. Walking, jogging, cycling, or swimming can release the tension caused by stressors. And learning relaxation techniques can have healthful benefits. Exercise can be thought of as preventative health care; promoting exercise for the 78 million “baby boomers” may be one of the best ways to reduce health care costs and improve quality of life (Shure & Cahan, 1998).
Nutrition
Nutritional concerns: Aging brings about a reduction in the number of calories a person requires. Many Americans respond to weight gain by dieting. However, eating less does not typically mean eating right and people often suffer vitamin and mineral deficiencies as a result. Very often, physicians will recommend vitamin supplements to their middle-aged patients.
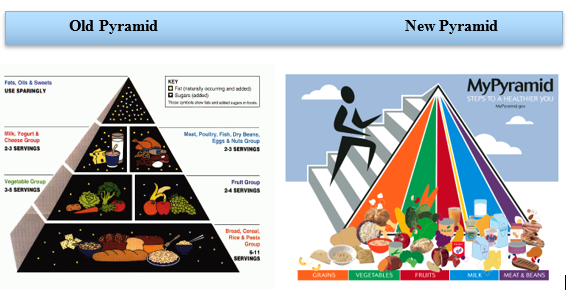
The new food pyramid: The ideal diet is one low in fat, sugar, high in fiber, low in sodium, and cholesterol. In 2005, the Food Pyramid, a set of nutritional guidelines established by the U. S. Government was updated to accommodate new information on nutrition and to provide people with guidelines based on age, sex, and activity levels.
 The ideal diet is also low in sodium (less than 2300 mg per day). Sodium causes fluid retention which may, in turn, exacerbate high blood pressure. The ideal diet is also low in cholesterol (less than 300 mg per day). The ideal diet is also one high in fiber. Fiber is thought to reduce the risk of certain cancers and heart disease. Finally, an ideal diet is low in sugar. Sugar is not only a problem for diabetics; it is also a problem for most people. Sugar satisfies the appetite but provides no protein, vitamins, or minerals. It provides empty calories. High starch diets are also a problem because starch is converted to sugar in the body. A 1-2 ounce serving of red wine (or grape juice) can have beneficial effects as well. Red wine can increase “good cholesterol” or HDLs (high-density lipoproteins) in the blood and provides antioxidants important to combating aging.
The ideal diet is also low in sodium (less than 2300 mg per day). Sodium causes fluid retention which may, in turn, exacerbate high blood pressure. The ideal diet is also low in cholesterol (less than 300 mg per day). The ideal diet is also one high in fiber. Fiber is thought to reduce the risk of certain cancers and heart disease. Finally, an ideal diet is low in sugar. Sugar is not only a problem for diabetics; it is also a problem for most people. Sugar satisfies the appetite but provides no protein, vitamins, or minerals. It provides empty calories. High starch diets are also a problem because starch is converted to sugar in the body. A 1-2 ounce serving of red wine (or grape juice) can have beneficial effects as well. Red wine can increase “good cholesterol” or HDLs (high-density lipoproteins) in the blood and provides antioxidants important to combating aging.
Coping
Stress Management: Around three-quarters of adults (76%) said they have experienced health impacts due to stress in the prior month (American Psychological Association, 2022). Given that the sources of our stress are often difficult to change (e.g., personal finances, current job), a number of interventions have been designed to help reduce the aversive responses to duress, especially related to health. For example, relaxation activities and forms of meditation are techniques that allow individuals to reduce their stress via breathing exercises, muscle relaxation, and mental imagery. Physiological arousal from stress can also be reduced via biofeedback, a technique where the individual is shown bodily information that is not normally available to them (e.g., heart rate), and then taught strategies to alter this signal. This type of intervention has even shown promise in reducing heart and hypertension risk, as well as other serious conditions (Moravec, 2008; Patel et al., 1981). Reducing stress does not have to be complicated. For example, exercise is a great stress reduction activity (Salmon, 2001) that has a myriad of health benefits.
Coping Strategies: Coping is often classified into two categories: Problem-focused coping or emotion-focused coping (Carver et al., 1989). Problem-focused coping is thought of as actively addressing the event that is causing stress in an effort to solve the issue at hand. For example, say you have an important exam coming up next week. A problem-focused strategy might be to spend additional time over the weekend studying to make sure you understand all of the material. Emotion-focused coping, on the other hand, regulates the emotions that come with stress. In the above examination example, this might mean watching a funny movie to take your mind off the anxiety you are feeling. In the short term, emotion-focused coping might reduce feelings of stress, but problem-focused coping seems to have the greatest impact on mental wellness (Billings & Moos, 1981; Herman-Stabl et al., 1995). That being said, when events are uncontrollable (e.g., the death of a loved one), emotion-focused coping directed at managing your feelings, at first, might be the better strategy. Therefore, it is always important to consider the match of the stressor to the coping strategy when evaluating its plausible benefits.
Cognitive Development in Midlife (Ob 10)
Brain Functioning
The brain at midlife has been shown to not only maintain many of the abilities of young adults but also gain new ones. Some individuals in middle age actually have improved cognitive functioning (Phillips, 2011). The brain continues to demonstrate plasticity and rewires itself in middle age based on experiences. Research has demonstrated that older adults use more of their brains than younger adults. In fact, older adults who perform the best on tasks are more likely to demonstrate bilateralization than those who perform worst. Additionally, the amount of white matter in the brain, which is responsible for forming connections among neurons, increases into the 50s before it declines.
Emotionally, the middle-aged brain is calmer, less neurotic, more capable of managing emotions, and better able to negotiate social situations (Phillips, 2011). Older adults tend to focus more on positive information and less on negative information than those younger. In fact, they also remember positive images better than those younger. Additionally, the older adult’s amygdala responds less to negative stimuli. Lastly, adults in middle adulthood make better financial decisions, which seems to peak at age 53, and show better economic understanding. Although greater cognitive variability occurs among middle adults when compared to those both younger and older, those in midlife with cognitive improvements tend to be more physically, cognitively, and socially active.
Brain Health & Diet
As general health concerns increase in midlife, many people wonder how to maintain brain health and prevent cognitive decline, dementia, or illnesses like Alzheimer’s disease. Researchers have investigated the connection between brain health and various lifestyle factors, including diet. The Mediterranean diet—high in fruit, vegetables, grains, and olive oil and low in red meat and processed foods—has also been associated with protecting healthy brain functioning. In particular, the brains of adults following this eating approach are less likely to exhibit the accumulation of plaques in the brain that lead to cognitive decline and Alzheimer’s disease (Agarwal et al., 2023).
Many aspects of the Mediterranean diet can be more affordable than less healthy food choices. For example, protein sources such as lentils and chickpeas are often cheaper than meat-based proteins. However, other food choices may be more costly, such as using olive oil instead of other sources of fat. Check out this article about more affordable ways to eat the Mediterranean way to learn what to prioritize on your shopping list.
Information processing
As we age, working memory, or our ability to simultaneously store and use information, becomes less efficient (Craik & Bialystok, 2006). The ability to process information quickly also decreases with age. This slowing of processing speed may explain age differences on many different cognitive tasks (Salthouse, 2004). Some researchers have argued that inhibitory functioning, or the ability to focus on certain information while suppressing attention to less pertinent information, declines with age and may explain age differences in performance on cognitive tasks (Hasher & Zacks, 1988).
With age, systematic declines are observed on cognitive tasks requiring self-initiated, effortful processing, without the aid of supportive memory cues (Park, 2000). In middle age comment about becoming forgetful, yet this is likely due to cognitive overload associated with the responsibilities of parenting, looking after aging parents, maintaining a career, and so on (Mayo Clinic Health System, 2022). Research has not shown middle age people seem to generally function similarly to young adults in terms of memory (Salthouse, 2012).
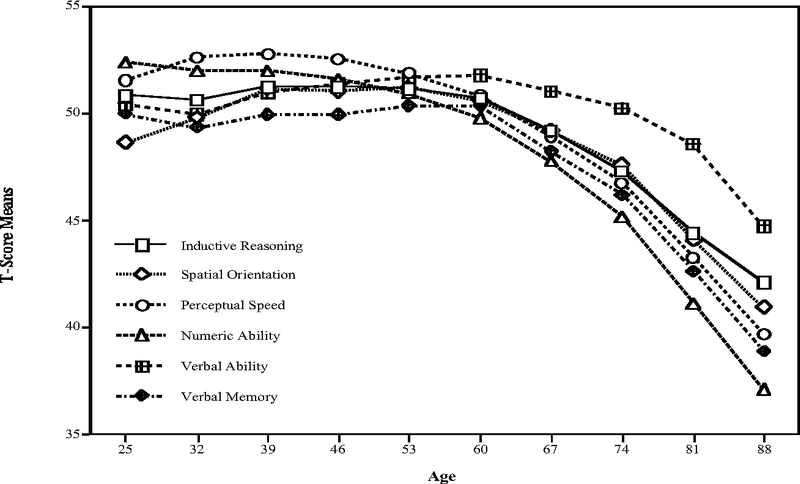
We will discuss more about memory changes in the next chapter, but we can examine memory changes through longitudinal research (tracking the same individuals over time). The Seattle Longitudinal Study has tracked the cognitive abilities of adults since 1956. Every seven years the current participants are evaluated and new individuals are also added. Approximately 6000 people have participated thus far, and 26 people from the original group are still in the study today. Current results demonstrate that middle-aged adults perform better on four out of six cognitive tasks than those same individuals did when they were young adults. Verbal memory, spatial skills, inductive reasoning (generalizing from particular examples), and vocabulary increase with age until one’s 70s (Schaie, 2005; Willis & Shaie, 1999). However, numerical computation and perceptual speed decline in middle and late adulthood.
We also see that tacit knowledge and other types of practical thought skills increase with age. Tacit knowledge is pragmatic or practical and learned through experience rather than explicitly taught. It might be thought of as “know-how” or “professional instinct.” It is referred to as tacit because it cannot be codified or written down. It does not involve academic knowledge, rather it involves being able to use skills and to problem-solve in practical ways. Tacit knowledge can be understood in the workplace and by blue-collar workers such as carpenters, chefs, and hairdressers.
Plasticity of Intelligence
Prior research on cognition and aging has been focused on comparing young and old adults and assuming that midlife adults fall somewhere in between. But some abilities may decrease while others improve during midlife. The concept of plasticity means that intelligence can be shaped by experience. Intelligence is influenced by culture, social contexts, and personal choices as much as by heredity and age. In fact, there is new evidence that mental exercise or training can have lasting benefits (National Institutes of Health, 2007). We explore aspects of midlife intelligence below.
Crystalized and Fluid Intelligence
One distinction in specific intelligences noted in adulthood is between fluid intelligence, which refers to the capacity to learn new ways of solving problems and performing activities quickly and abstractly, and crystallized intelligence, which refers to the accumulated knowledge of the world, we have acquired throughout our lives (Salthouse, 2004). These intelligences are distinct, and crystallized intelligence increases with age, while fluid intelligence tends to decrease with age (Horn et al., 1981; Salthouse, 2004). There is a general acceptance that fluid intelligence decreases continually from the 20s, but that crystallized intelligence continues to accumulate.
Fluid intelligence refers to information processing abilities (e.g., logical reasoning, remembering lists, spatial ability, and reaction time). Crystallized intelligence encompasses abilities that draw upon experience and knowledge (e.g., vocabulary tests, solving number problems, and understanding texts). Crystallized intelligence includes verbal memory, spatial skills, inductive reasoning (generalizing from particular examples), and vocabulary — all of which increase with age (Willis & Shaie, 1999). Research demonstrates that older adults have more crystallized intelligence as reflected in semantic knowledge, vocabulary, and language. As a result, adults generally outperform younger people on measures of history, geography, and even on crossword puzzles, where this information is useful (Salthouse, 2004). It is this superior knowledge, combined with a slower and complete processing style, along with a more sophisticated understanding of the workings of the world around them, which gives older adults the advantage of “wisdom” over the advantages of fluid intelligence which favor the young (Baltes et al., 1999; Scheibe et al., 2009).
The differential changes in crystallized versus fluid intelligence help explain why older adults do not necessarily show poorer performance on tasks that also require experience or expertise (i.e., crystallized intelligence), although they show poorer memory overall. With age often comes expertise, and research has pointed to areas where aging experts perform as well or better than younger individuals. For example, older typists were found to compensate for age-related declines in speed by looking farther ahead at printed text (Salthouse, 1984). Compared to younger players, older chess experts are able to focus on a smaller set of possible moves, leading to greater cognitive efficiency (Charness, 1981). A young chess player may think more quickly, for instance, but a more experienced chess player has more knowledge to draw on. Older pilots show declines in processing speed and memory capacity, but their overall performance seems to remain intact. According to Phillips (2011) researchers tested pilots age 40 to 69 as they performed on flight simulators. Older pilots took longer to learn to use the simulators, but performed better than younger pilots at avoiding collisions. Accrued knowledge of everyday tasks, such as grocery prices, can help older adults to make better decisions than young adults (Tentori et al., 2001).
Formal Operational Thought (Piaget revisited)
Remember formal operational thought? Formal operational thought involves being able to think abstractly; however, this ability does not apply to all situations or subjects. Formal operational thought is influenced by experience and education. Some adults lead patterned, orderly lives in which they are not challenged to think abstractly about their world. Many adults do not receive any formal education and are not taught to think abstractly about situations they have never experienced. Nor are they exposed to conceptual tools used to formally analyze hypothetical situations. Those who do think abstractly, in fact, may be able to do so more easily in some subjects than others. For example, English majors may be able to think abstractly about literature, but be unable to use abstract reasoning in physics or chemistry. Abstract reasoning in a particular field requires a knowledge base that we might not have in all areas. So, our ability to think abstractly depends to a large extent on our experiences. As discussed previously, adults tend to think in more practical terms than do adolescents. Although they may be able to use abstract reasoning when they approach a situation and consider possibilities, they are more likely to think practically about what is likely to occur.
Flow is the mental state of being completely present and fully absorbed in a task (Csikszentmihalyi, 1990). When in a state of flow, the individual is able to block outside distractions and the mind are fully open to producing. Additionally, the person is achieving great joy or intellectual satisfaction from the activity and accomplishing a goal. Further, when in a state of flow, the individual is not concerned with extrinsic rewards. Csikszentmihalyi (1996) used his theory of flow to research how some people exhibit high levels of creativity as he believed that a state of flow is an important factor in creativity (Kaufman & Gregoire, 2016). Other characteristics of creative people identified by Csikszentmihalyi (1996) include curiosity and drive value for intellectual endeavors, and an ability to lose our sense of self and feel a part of something greater. In addition, he believed that the tortured creative person was a myth and that creative people were very happy with their lives. According to Nakamura and Csikszentmihalyi (2002) people describe flow as the height of enjoyment. The more they experience it, the more they judge their lives to be gratifying. The qualities that allow for flow are well-developed in middle adulthood.
Learning in Older Adults (Ob 11)
Midlife adults in the United States often find themselves in classrooms. Whether they enroll in school to sharpen particular skills, to retool and reenter the workplace, or to pursue interests that have previously been neglected, these students tend to approach teach differently than do younger college students (Knowles et al., 1998).
The mechanics of cognition, such as working memory and speed of processing, gradually decline with age. However, they can be easily compensated for through the use of higher-order cognitive skills, such as forming strategies to enhance memory or summarizing and comparing ideas rather than relying on rote memorization (Lachman, 2004). An 18-year-old college student may focus more on rote memorization in studying for tests. They may be able to memorize information more quickly than an older student, but not have as thorough a grasp on the meaning of that information. Older students may take a bit longer to learn the material, but are less likely to forget it quickly. Adult learners tend to look for relevance and meaning when learning information. Older adults have the hardest time learning material that is meaningless or unfamiliar. They are more likely to ask themselves, “What does this mean?” or “Why is this important?” when being introduced to information or when trying to concepts or facts. Older adults are more task-oriented learners and want to organize their activity around problem-solving. They see the instructor as a resource person rather than the “expert” and appreciate having their life experience recognized and incorporated into the material being covered. This type of learning is more easily accomplished if adequate time is allowed for mastering the material. Keeping distractions at a minimum and studying when rested and energetic enhances adult learning.
To address the educational needs of those over 50, The American Association of Community Colleges (2016) developed the Plus 50 Initiative that assists community college in creating or expanding programs that focus on workforce training and new careers for the plus-50 population. Since 2008 the program has provided grants for programs to 138 community colleges affecting over 37, 000 students. The participating colleges offer workforce training programs that prepare 50 plus adults for careers in such fields as early childhood educators, certified nursing assistants, substance abuse counselors, adult basic education instructors, and human resources specialists. These training programs are especially beneficial as 80% of people over the age of 50 say they will retire later in life than their parents or continue to work in retirement, including in a new field.
Gaining Expertise: The Novice and the Expert (Ob 9)
We discussed the benefits of expertise with age and now we will discuss more about expert thought. When we work extensively in an area, we may gain expertise. Consider the study skills of a seasoned student versus a new student or a new nurse versus an experienced nurse. One of the major differences is that the new one operates as a novice while the seasoned student or nurse performs more like an expert. An expert has a different approach to learning and problem-solving than does a novice or someone new to a field. While a novice tends to rely on formal procedures or guidelines, the expert relies more on intuition and is more flexible in solving problems. A novice’s performance tends to be more conscious and methodical than experts. An expert tends to perform actions in a more automatic fashion. An expert cook, for example, may be able to prepare a difficult recipe but not really describe how they did it. The novice cook might rigidly adhere to the recipe, hanging on every word and measurement. The expert also has better strategies for tackling problems than does a novice.
Expertise refers to specialized skills and knowledge that pertain to a particular topic or activity. In contrast, a novice is someone who has limited experiences with a particular task. Everyone develops some level of “selective” expertise in things that are personally meaningful to them, such as making bread, quilting, computer programming, or diagnosing illness. Expert thought is often characterized as intuitive, automatic, strategic, and flexible.
- Intuitive: Novices follow particular steps and rules when problem-solving, whereas experts can call upon a vast amount of knowledge and past experience. As a result, their actions appear more intuitive than formulaic. A novice cook may slavishly follow the recipe step by step, while a chef may glance at recipes for ideas and then follow her own procedure.
- Automatic: Complex thoughts and actions become more routine for experts. Their reactions appear instinctive over time, and this is because expertise allows us to process information faster and more effectively (Crawford & Channon, 2002).
- Strategic: Experts have more effective strategies than non-experts. For instance, while both skilled and novice doctors generate several hypotheses within minutes of an encounter with a patient, the more skilled clinicians’ conclusions are likely to be more accurate. In other words, they generate better hypotheses than the novice. This is because they are able to discount misleading symptoms and other distractors and hone in on the most likely problem the patient is experiencing (Norman, 2005).
- Flexible: Experts in all fields are more curious and creative; they enjoy a challenge and experiment with new ideas or procedures. The only way for experts to grow in their knowledge is to take on more challenging, rather than routine tasks.
Expertise takes time. It is a long process resulting from experience and practice (Ericsson et al., 2006). Middle-aged adults, with their store of knowledge and experience, are likely to find that when faced with a problem they have likely faced something similar before. This allows them to ignore the irrelevant and focus on the important aspects of the issue. Expertise is one reason why many people often reach the top of their career in middle adulthood. However, expertise cannot fully make-up for all losses in general cognitive functioning as we age. The superior performance of older adults in comparison to younger novices appears to be task specific (Charness & Krampe, 2006). As we age, we also need to be more deliberate in our practice of skills in order to maintain them. Charness and Krampe (2006) in their review of the literature on aging and expertise, also note that the rate of return for our effort diminishes as we age. In other words, increasing practice does not recoup the same advances in older adults as similar efforts do at younger ages.
Psychosocial Development during Midlife
What do you think is the happiest stage of life? What about the saddest stages? Perhaps surprisingly, Blanchflower & Oswald (2008) found that reported levels of unhappiness and depressive symptoms peak in the early 50s for men in the U.S., and interestingly, the late 30s for women. In Western Europe, minimum happiness is reported around the mid 40s for both men and women, albeit with some significant national differences. Stone et al. (2017) reported a precipitous drop in perceived stress in men in the U.S. from their early 50s. There is now a view that “older people” (50+) may be “happier” than younger people, despite some cognitive and functional losses. This is often referred to as “the paradox of aging.” Positive attitudes to the continuance of cognitive and behavioral activities, interpersonal engagement, and their vitalizing effect on human neural plasticity, may lead not only to more life, but to an extended period of both self-satisfaction and continued communal engagement.
Midlife crisis? (Ob 10)
Remember Levinson’s theory from the last chapter? Levinson found that the men he interviewed sometimes had difficulty reconciling the “dream” they held about the future with the reality they now experience. “What do I really get from and give to my wife, children, friends, work, community-and self?” a man might ask (Levinson, 1978, p. 192). Tasks of the midlife transition include 1) ending early adulthood; 2) reassessing life in the present and making modifications if needed, and 3) reconciling “polarities” or contradictions in one’s sense of self. Perhaps, early adulthood ends when a person no longer seeks adult status but feels like a full adult in the eyes of others. This ‘permission’ may lead to different choices in life; choices that are made for self-fulfillment instead of social acceptance. While people in their early 20s may emphasize how old they are (to gain respect, to be viewed as experienced), by the time people reach their 40s, they tend to emphasize how young they are. (Few 40-year-olds cut each other down for being so young: “You’re only 43? I’m 48!!”)
This new perspective on time brings about a new sense of urgency to life. The person becomes focused more on the present than the future or the past. The person grows impatient at being in the “waiting room of life” postponing doing the things they have always wanted to do. Now is the time. If it’s ever going to happen, it better happen now. A previous focus on the future gives way to an emphasis on the present. Neugarten (1968) notes that in midlife, people no longer think of their lives in terms of how long they have lived. Rather, life is thought of in terms of how many years are left. If an adult is not satisfied at midlife, there is a new sense of urgency to start to make changes now.

Changes may involve ending a relationship or modifying one’s expectations of a partner. These modifications are easier than changing the self (Levinson, 1978). Midlife is a period of transition in which one holds earlier images of the self while forming new ideas about the self of the future. Greater awareness of aging accompanies feelings of youth. And the harm that may have been done previously in relationships haunts new dreams of contributing to the well-being of others. These polarities are the quieter struggles that continue after outward signs of “crisis” have gone away.
It’s important to note that the concept of a midlife crisis is complex and not universally accepted. Although Levinson characterized midlife as a time of developmental crisis research suggests that most people in the United States today do not experience a midlife crisis and that, in fact, many women find midlife a freeing, satisfying period. Results of a 10-year study conducted by the MacArthur Foundation Research Network on Successful Midlife Development, based on telephone interviews with over 3,000 midlife adults suggest that the years between 40 and 60 are ones marked by a sense of well-being. Only 23 percent of their participants reported experiencing a midlife crisis. The crisis tended to occur among the highly educated and was triggered by a major life event rather than out of fear of aging (Research Network on Successful Midlife Development, 2007). The Midlife in the United States Study, MIDUS, survey also shows that a crisis is not a typical midlife phenomenon. Certainly, some do have a crisis in midlife, with between 10 and 20% in the U.S. reporting one (Wethington, 2000). Of those who say they have had a midlife crisis, about half say it involves inner turmoil or angst associated with getting older. For the rest, it is tied to events such as divorce, job loss, or health problems, which can occur at any age period (Wethington, 2000). Those who do experience a crisis in midlife are usually those who have upheavals at other times in their lives, and these individuals seem to be driven more by a neurotic personality than advancing age (Lachman, 2004). Nevertheless, sales of products designed to make one feel younger and “over the hill” birthday parties with black balloons and banners abound.
Goal Perspective Taking
One of the reasons the men in Levinson’s study became concerned about their life was because it had not followed the course they had envisioned. Shapiro (2006) offers an alternative to linear thinking about the future and career paths. Many plan their futures by using a map. They have a sense of where they are and where they want to be and form strategies to get from point A to point B. While this seems perfectly logical, Shapiro suggests that following a map closes one to opportunities for the future and provides a standard by which all actual events may fall short. Life, then, is evaluated by how closely actual life events have followed the map. If so, all is well. If not, a feeling of frustration and failure creeps in. Shapiro suggests using a compass rather than a map as one’s guide. A compass indicates a direction but does not provide a destination. So, an individual has direction and areas of interest that guide decision-making but does not know the outcome. (Many of us do not know the outcome-even when we follow a map!) This approach opens a person up to possibilities that often occur by chance and frees one from being stressed or devastated if a preset destination is not reached by a certain time. And more importantly, compass-guided living focuses a person’s attention on the process of the journey and helps them appreciate all of their experiences along the way.
![]()
What do you think? How many of your plans were mapped out previously? Could you be happy knowing that you do not know where you will be 5 years from now?

Finding Gender Identity at Midlife: The Story of ErikaThe late 40s brought about dramatic change in Erika’s life. Erika is a transsexual who began the process of transitioning from male to female at about age 48. Since about age 8, Erika (then Richard) felt that he was more feminine than masculine. An impromptu game of “dress up” with a girl who lived in the neighborhood left Richard feeling a sense of connection and ‘rightness’ he had not before experienced. Through the years, dressing up and wearing make-up provided comfort and relief as well as the anxiety of possibly being discovered. Richard married and pursued a career in the military and later as a geologist, two very masculine careers, but all the while felt out of place in a masculine world. Through the years, discomfort gave rise to depression and thoughts of suicide. “I felt like some sick, weird person.” Not knowing what was wrong and not having anyone to talk to was very difficult. Erika finally found out what was wrong after searching the internet. First, she looked up “transvestite.” “Is that what I am?” she wondered. But these descriptions did not apply. Finally, she learned about gender dysphoria, marked by a feeling of discomfort and disconnection between one’s sense of self and biological gender. Eventually, Richard got the courage to tell his wife. Her response was, “you’re killing my husband,” to which he replied, “He would have died anyway.” The couple separated after 24 years of marriage. After several months, however, the couple got back together. “We were just too good of friends to break up.” But her wife did not want to see it, initially. “I would get dressed in the garage or dress like a man from the waist up and then stop behind a grocery store and finish changing before I got to my destination.” Erika found a psychologist in the phone book and began treatment under the Harry Benjamin standard of care. This care requires that an individual be identified as transsexual by two psychologists, and lives completely as a member of the other sex for one year before beginning surgical and hormonal treatments. Erika’s surgery cost about $30,000. Hormone therapy and electrolysis cost far more. Now in their 30th year together, Erika, and her wife live under the same roof, but no longer share a bedroom. Erika now has full status through the state and government as a female. And her wife is a warm, accepting, roommate. “The day that she yelled from her bedroom, ‘do you have any pantyhose’ was an important one.” And seeing her lipstick on the rim of a wine glass created a feeling of congruence for Erika. Erika could now be Erika. |
Erikson’s Theory (Ob 12)
According to Erikson, midlife adults face the crisis of generativity vs. stagnation. According to Erikson (1982) generativity encompasses procreativity, productivity, and creativity. This stage includes the generation of new beings, new products, and new ideas, as well as self-generation concerned with further identity development. This involves looking at one’s life while asking the question, “Am I doing anything worthwhile? Is anyone going to know that I was here? What am I contributing to others?” If not, a feeling of being stuck or stagnated may result. This discomfort can motivate a person to redirect energies into more meaningful activities. It is important to make revisions here so that in later life, one may feel a sense of pride and accomplishment and feel content with the choices that have been made.
Erikson believed that the stage of generativity, during which one established a family and career, was the longest of all the stages. Erikson believed that those in middle adulthood should “take care of the persons, the products, and the ideas one has learned to care for” (Erikson, 1982, p. 67). Erikson further argued that generativity occurred best after the individual had resolved issues of identity and intimacy (Peterson & Duncan, 2007). Individuals at midlife are primarily concerned with leaving a positive legacy of themselves, and according to Erikson (1950) parenthood is the primary generative type. Erikson understood that work and family relationships may be in conflict due to the obligations and responsibilities of each, but he believed it was overall a positive developmental time. In addition to being parents and working, Erikson also described individuals being involved in the community during this stage. A sense of stagnation occurs when one is not active in generative matters, however, stagnation can motivate a person to redirect energies into more meaningful activities.

Erikson believed that those in middle adulthood should “take care of the persons, the products, and the ideas one has learned to care for” (Erikson, 1982, p. 67). Further, Erikson believed that the strengths gained from the six earlier stages are essential for the generational task of cultivating strength in the next generation. Erikson further argued that generativity occurred best after the individual had resolved issues of identity and intimacy (Peterson & Duncan, 2007).
Research has demonstrated that generative adults possess many positive characteristics, including good cultural knowledge and healthy adaptation to the world (Peterson & Duncan, 2007). Using the Big 5 personality traits, generative women and men scored high on conscientiousness, extraversion, agreeableness, openness to experience, and low on neuroticism (de St. Aubin & McAdams, 1995; Peterson et al., 1997). Additionally, women scoring high in generativity at age 52, were rated high in positive personality characteristics, satisfaction with marriage and motherhood, and successful aging at age 62 (Peterson & Duncan, 2007). Similarly, men rated higher in generativity at midlife were associated with stronger global cognitive functioning (e.g., memory, attention, calculation), stronger executive functioning (e.g., response inhibition, abstract thinking, cognitive flexibility), and lower levels of depression in late adulthood (Malone et al., 2016).
Erikson (1982) indicated that at the end of this demanding stage, individuals might withdraw as generativity is no longer expected in late adulthood. This releases elders from the task of care taking or working. However, not feeling needed or challenged may result in stagnation, and consequently one should not fully withdraw from generative tasks as they enter Erikson’s last stage in late adulthood.
Personality in Midlife (Ob 14)
Does personality change in midlife? If you think about your parents or other adults you’ve known for some time, you might notice that some seem to remain much the same, while others show new sides of themselves as they age. Some theorists argue that personality becomes more stable in middle adulthood, especially compared to the changes seen in adolescence and early adulthood. Research, including findings from the MIDUS project and other longitudinal studies, generally supports this view: most adults maintain consistent patterns in the Big Five personality traits—openness, conscientiousness, extraversion, agreeableness, and neuroticism—over time (Lucas & Donnellan, 2011; Roberts & Mroczek, 2008). This stability is thought to be rooted in both biological heredity and gene-environment correlations, where individuals seek out environments that reinforce their natural dispositions. However, contemporary research also acknowledges that while many people’s personalities are relatively stable, others do experience meaningful changes, often in response to significant life events or shifting roles.
At the same time, middle adulthood is a period of ongoing personality development as adults adapt to new roles at home, work, and in their communities. Whether it’s the development of new personal qualities with age, or life changes themselves that foster growth, this stage is often marked by increasing socioemotional maturity. For example, conscientiousness tends to increase as adults take on more responsibilities, and research shows that adults in midlife are more likely to prioritize generativity, altruism, and concern for future generations—reflecting Erikson’s virtue of care. Longitudinal studies reveal average increases in agreeableness and conscientiousness, mixed findings for openness, a reduction in neuroticism (especially in women), and little change in extraversion (Damian et al., 2019; Roberts, Wood & Caspi, 2008). These changes, sometimes referred to as “maturation,” may be both a cause and effect of other psychosocial developments during this stage of life. Importantly, traits like conscientiousness have been linked to positive life outcomes, including job success, health, and longevity.
The interplay between stability and change in personality during midlife is further shaped by the goodness-of-fit: adults are most satisfied and successful when their interests, goals, and traits align with their environments. Positive alignment can foster growth and well-being, while misalignment or negative experiences, such as family-work conflict, can predict anxiety and less adaptive personality changes. Yet growth can also emerge from adversity; for example, adults who use goal-oriented coping in response to health fears may adopt healthier behaviors, and cancer survivors often report increased personal mastery. Ultimately, personality in midlife reflects both enduring patterns and the capacity for meaningful growth and adaptation.
Productivity at home and family (Ob 14)
Family relationships: Younger and older adults tend to experience more spouse-related stress than do midlife adults. Midlife adults often have overload stressors such as having too many demands placed on them by children or due to financial concerns. Parents adjust to launching their children into lives of their own during this time. Some parents who feel uncomfortable about their children leaving home may actually precipitate a crisis to keep it from happening or push their child out too soon (Anderson & Sabatelli, 2007). When children leave the house this is known as the empty nest. The empty nest, or post-parental period (Dennerstein et al., 2002), refers to the time period when children are grown up and have left home. For most parents this occurs during midlife. This time is recognized as a “normative event” as parents are aware that their children will become adults and eventually leave home (Mitchell & Lovegreen, 2009). The empty nest creates complex emotions, both positive and negative, for many parents. Some theorists suggest this is a time of role loss for parents, others suggest it is one of role strain relief (Bouchard, 2013). A number of studies in China suggest that empty-nesters, especially in more rural areas of China, report greater loneliness and depression than their counterparts with children still at home (Wu et al., 2010). Family support for the elderly by their children is a cherished Chinese tradition (Wong & Leung, 2012).
It can be typical for those in midlife to be carrying for a parent while still supporting their grown children. The sandwich generation refers to adults who have at least one parent age 65 or older and are either raising their own children or providing support for their grown children. According to a recent Pew Research survey, 47% of middle-aged adults are part of this sandwich generation (Parker & Patten, 2013). In addition, 15% of middle-aged adults are providing financial support to an older parent while raising or supporting their own children. According to the same survey, almost half (48%) of middle-aged adults, have supported their adult children in the past year, and 27% are the primary source of support for their grown children.
Adult children typically maintain frequent contact with their parents if for no other reason, for money and advice. Attitudes toward one’s parents may become more accepting and forgiving as parents are seen in a more objective way-as people with good points and bad. And, like adults, children can continue to be subjected to criticism, ridicule, and abuse at the hand of parents. How long are we “adult children”? For as long as our parents are living, we continue in the role of son or daughter. (I had a neighbor in her nineties who would tell me her “boys” were coming to see her this weekend. Her boys were in their 70s-but they were still her boys!) But after one’s parents are gone, the adult is no longer a child; as one 40-year-old man explained after the death of his father, “I’ll never be a kid again.” And adult children who are returning after having lived independently outside the home, known as boomerang kids, may return home to live temporarily after divorces, for mental health issues, or if they lose employment. Parker (2012) found that 63% of 18 to 34 year- olds know someone who has returned to live with their parents (Sandberg-Thoma et al., 2015).
In previous chapters you have read about the effects that parents have on their children’s development, but remember that this relationship is bidirectional. The problems faced by children, even when those children are adults, influence the lives of their parents. Greenfield and Marks (2006) found in their study of middle-aged parents and their adult children, those parents whose children were dealing with personal problems reported more negative affect, lower self-acceptance, poorer parent-child interactions, and more family relationship stress. The more problems the adult children were facing, the worse the lives and emotional health of their parents, with single parents faring the worst.

Being a midlife child sometimes involves kinkeeping; organizing events and communication in order to maintain family ties. Kin-keepers are often midlife daughters (they are the person who tells you what food to bring to a gathering or makes arrangement for a family reunion), but kin-keepers can be midlife sons as well. Leach and Braithwaite found that 86% of their respondents named a woman as their family’s kin-keeper, and Brown and DeRycke found that mothers, maternal grandmothers, and paternal grandmothers were more likely to be a family’s kinkeeper than were fathers, young adult children, and grandfathers combined. Brown and DeRycke also found that among young adults, women were more likely to be a kin-keeper than were young adult men. Kinkeeping can be a source of distress when it interferes with other obligations (Gerstel & Gallagher, 1993). Gerstel and Gallagher found that on average, kin-keepers provide almost a full week of work each month to kin-keeping (almost 34 hours). They also found that the more activities the kin-keeper took on, and the more kin they helped the more stress and higher the levels of depression a kin-keeper experienced. However, unlike other studies on kin-keeping, Gerstel and Gallagher also included a number of activities that would be considered more “caregiving,” such as providing transportation, making repairs, providing meals, etc. in addition to the usual activities of kin-keeping.
Caregiving of a disabled child, spouse, or other family member is part of the lives of some midlife adults. Overall, one major source of stress is that of trying to balance caregiving with meeting the demands of work away from home. Caregiving can have both positive and negative consequences that depend in part on the gender of the caregiver and the person receiving the care. Men and women express greater distress when caring for a spouse than when caring for other family members. Men who care are providing care for a spouse are more likely to experience greater hostility but also more personal growth than non-caregiving males. Men who are caring for disabled children express having more positive relationships with others. Women experience more positive relationships with others and greater purpose in life when caring for parents either in or outside of their home. But women who are caring for disabled children may experience poorer health and greater distress as a result (Marks, 1998).
According to the National Alliance for Caregiving (2022), 53 million Americans provide unpaid caregiving. The typical caregiver is a 49 year-old female currently caring for a 69 year-old female who needs care because of a long-term physical condition. Currently 25% of adult children, mainly baby boomers, provide personal or financial care to a parent (Metlife, 2011). Daughters are more likely to provide basic care and sons are more likely to provide financial assistance. Adult children 50+ who work and provide care to a parent are more likely to have fair or poor health when compared to those who do not provide care. Some adult children choose to leave the work force, however, the cost of leaving the work force early to care for a parent is high. For females, lost wages and social security benefits equals $324,044, while for men it equals $283,716 (Metlife, 2011). This loss can jeopardize the adult child’s financial future. Consequently, there is a need for greater workplace flexibility for working caregivers.
Families play a crucial role in our overall development and happiness. They can support and validate us, but they can also criticize and burden us. For better or worse, we all have a family. In closing, here are strategies you can use to increase the happiness of your family:
- Teach morality—fostering a sense of moral development in children can promote well-being (Damon, 2004).
- Savor the good—celebrate each other’s successes (Gable et al., 2006).
- Use the extended family network—family members of all ages, including older siblings and grandparents, who can act as caregivers can promote family well-being (Armstrong et al., 2005).
- Create family identity—share inside jokes, fond memories, and frame the story of the family (McAdams, 1993).
- Forgive—Don’t hold grudges against one another (McCullough et al., 1997).
The National Alliance for Caregiving seeks to “support and empower family caregivers to thrive at home, work, and life” through research, policy analysis, and advocacy. To increase the visibility of caregivers in the United States, they collect and share stories of the lived experiences of real people. Read some of these stories or share your own on their website.
Intimate Relationships
Single or Spouse-free? The number of adults who remain single has continued to increase. As of 2022, singles represent almost half (49.3%) of American households (U.S. Census Bureau). Nearly 1 in 5 adults between the ages of 45 and 54 have never married, and over 1 in 10 adults aged 55 and older have never married. While some of these individuals may be living with a partner, the trend towards singlehood is clear. Singlehood has become an increasingly accepted lifestyle, and many singles are very happy with their status.
Many of the research findings of singles reveal that they are not all alike. Happiness with one’s status depends on whether the person is single by choice and whether the situation is permanent. Bella DePaulo’s (2014) research, along with that of others, has found that those who are married may be more satisfied with life than the divorced or widowed, but there is little difference between married and always single.
Online Dating: Montenegro (2003) surveyed over 3,000 singles aged 40–69, and almost half of the participants reported their most important reason for dating was to have someone to talk to or do things with. Additionally, sexual fulfillment was also identified as an important goal for many. Alterovitz & Mendelsohn (2013) reviewed online personal ads for men and women over age 40 and found that romantic activities and sexual interests were mentioned at similar rates among the middle-age and young-old age groups, but less for the old-old age group.
Marriage: Thirty-six countries (fewer than 20 percent of all countries across the globe) have legalized same-sex marriage as of 2024. It has been said that marriage can be the greatest source of happiness or pain in one’s life, depending on the relationship. Those who are in marriages can experience deeper happiness and pain than those who are unattached. All marriages are not alike and the same marriage between two people may change through the years. Pew Research indicated that 48% of adults age 45-54 are married; either in their first marriage (22%) or have remarried (26%). This makes marriage the most common relationship status for middle-aged adults in the United States. Marital satisfaction tends to increase for many couples in midlife as children are leaving home (Landsford et al., 2005). Not all researchers agree. They suggest that those who are unhappy with their marriage are likely to have gotten divorced by now, making the quality of marriages later in life only look more satisfactory (Umberson et al., 2005). Below we will look at how satisfaction with marriage is affected by the life cycle and two ways to characterizing marriages.
Marital satisfaction & the life cycle: Marital satisfaction has peaks and valleys during the course of the life cycle. Rates of happiness are highest in the years prior to the birth of the first child. It hits a low point with the coming of children. Relationships become more traditional and there are more financial hardships and stress in living. Then it begins to improve when children leave home. Children bring new expectations to the marital relationship. Two people, who are comfortable with their roles as partners, may find the added parental duties and expectations more challenging to meet. Some couples elect not to have children in order to have more time and resources for the marriage. These child-free couples are happy keeping their time and attention on their partners, careers, and interests.
Marital Communication (Ob 15)
Advice on how to improve one’s marriage is centuries old. One of today’s experts on marital communication is John Gottman. Gottman (1999) differs from many marriage counselors in his belief that having a good marriage does not depend on compatibility. Rather, the way that partners communicate with one another is crucial. At the University of Washington in Seattle, Gottman has measures the physiological responses of thousands of couples as they discuss issues of disagreement. Fidgeting in one’s chair, leaning closer to or further away from the partner while speaking, increases in respiration and heart rate are all recorded and analyzed along with videotaped recordings of the partners’ exchanges. Gottman believes he can accurately predict whether or not a couple will stay together by analyzing their communication. In marriages destined to fail, partners engage in the “marriage killers,” also known as the 4-horsemen: contempt, criticism, defensiveness, and stonewalling. Each of these undermines the politeness and respect that healthy marriages require. And stonewalling, or shutting someone out, is the strongest sign that a relationship is destined to fail.
Table. Gottman’s 4 horsemen and more positive approaches
| Gottman’s horsemen | Possible Solutions |
| Contempt: Attacking character | Make requests |
| Criticism: Ridicule or disrespect, thinking lesser | Appreciate and respect |
| Defensiveness: self-protection or retaliation, shifting to partner’s flaws | Accept responsibility |
| Stonewalling: withdraw from interaction, avoidance of conflict, turning away, acting busy | Self-soothe & reengage |
Adapted from Gottman (2017)

Divorce (Ob 16)
Livingston (2014) found that 27% of adults age 45 to 54 were divorced. Additionally, 57% of divorced adults were women. This reflects the fact that men are more likely to remarry than are women. Two-thirds of divorces are initiated by women (AARP, 2009). Most divorces take place within the first 5 to 10 years of marriage. This time line reflects people’s initial attempts to salvage the relationship. After a few years of limited success, the couple may decide to end the marriage. It used to be that divorce after having been married for 20 or more years was rare, but in recent years the divorce rate among more long-term marriages has been increasing. Brown and Lin (2013) note that while the divorce rate in the U.S. has declined since the 1990s, the rate among those 50 and older has doubled. They suggest several reasons for the “graying of divorce”. There is less stigma attached to divorce today than in the past. Some older women are out-earning their spouses, and thus may be more financially capable of supporting themselves, especially as most of their children have grown. Finally, given increases in human longevity, the prospect of living several more years or decades with an incompatible spouse may prompt middle-aged and older adults to leave the marriage.
Gottman and Levenson (2000) found that the divorces in early adulthood were more angry and conflictual, with each partner blaming the other for the failures in the marriage. In contrast, they found that at midlife divorces tended to be more about having grown apart, or a cooling off of the relationship. A survey by AARP (2009) found that men and women had diverse motivations for getting a divorce. Women reported concerns about the verbal and physical abusiveness of their partner (23%), drug/alcohol abuse (18%), and infidelity (17%). In contrast, men mentioned they had simply fallen out of love (17%), no longer shared interests or values (14%), and infidelity (14%). Both genders felt their marriage had been over long before the decision to divorce was made, with many of the middle-aged adults in the survey reporting that they stayed together because they were still raising children. Only 1 in 4 regretted their decision to divorce.
The effects of divorce are varied. Divorce at midlife is more stressful for women. In the AARP (2009) survey, 44% of middle-aged women mentioned financial problems after divorcing their spouse, in comparison only 11% of men reported such difficulties. However, a number women who divorce in midlife report that they used the experience to better themselves or grow emotionally (Hetherington & Kelly, 2002).
Dating Post-Divorce: Most divorced adults have dated by one year after filing for divorce (Anderson et al., 2004; Anderson & Greene, 2011). One in four recent filers report having been in or were currently in a serious relationship, and over half were in a serious relationship by one year after filing for divorce. Dating for adults with children can be more of a challenge. Courtships are shorter in remarriage than in first marriages. When couples are “dating”, there is less going out and more time spent in activities at home or with the children. So the couple gets less time together to focus on their relationship. Anxiety or memories of past relationships can also get in the way.
Post-divorce parents gatekeep, that is, they regulate the flow of information about their new romantic partner to their children, in an attempt to balance their own needs for romance with consideration regarding the needs and reactions of their children. Anderson et al. (2004) found that almost half (47%) of dating parents gradually introduce their children to their dating partner, giving both their romantic partner and children time to adjust and get to know each other. Many parents who use this approach do so to avoid their children having to keep meeting someone new until it becomes clearer that this relationship might be more than casual. It might also help if the adult relationship is on firmer ground so it can weather any initial push back from children when it is revealed. Forty percent are open and transparent about the new relationship at the outset with their children. Thirteen percent do not reveal the relationship until it is clear that cohabitation and or remarriage is likely. Anderson and colleagues suggest that practical matters influence which gatekeeping method parents may use. Parents may be able to successfully shield their children from a parade of suitors if there is reliable childcare available. The age and temperament of the child, along with concerns about the reaction of the ex-spouse, may also influence when parents reveal their romantic relationships to their children.
How Do Children Influence Recoupling/Repartnering?
Does having children affect whether a parent remarries? Goldscheider and Sassler (2006) found children residing with their mothers reduces the mothers’ likelihood of marriage, only with respect to marrying a man without children. One of the reasons for this is because women with children have less time and fewer resources for dating. Dating is difficult for a woman who has to find a babysitter, pay for a babysitter, and ‘come home on time’ if she is concerned about what her children think about her relationships. There is more guilt experienced about going out and finding the time and location for sexual intimacy can be problematic. Men may shy away from the responsibility of children or may find it difficult to get along with a girlfriend’s children. And parents may find it difficult to date someone who wants to change the relationship they have with their children. Sometimes, she may feel pulled in two directions as the children and the man in her life all seek attention and engage in power struggles to get it. Some women decide that it is easier to be single than to experience such divisions. (This can also be true for men whose dates try to establish their importance over the importance of the children.) Children usually remain central to a single parent’s life.
Having children in the home appears to increase single men’s likelihood of marrying a woman with children (Stewart et al., 2003). There is also some evidence that individuals who participated in a stepfamily while growing up may feel better prepared for stepfamily living as adults. Goldscheider and Kaufman (2006) found that having experienced family divorce as a child is associated with a greater willingness to marry a partner with children.
When children are present after divorce, one of the challenges the adults encounter is how much influence the child will have when selecting a new partner. Greene et al. (2003) identified two types of parents. The child- focused parent allows the child’s views, reactions, and needs to influence the repartnering. In contrast, the adult-focused parent expects that their child can adapt and should accommodate to parental wishes.
Anderson and Greene (2011) found that divorced custodial mothers identified as more adult focused tended to be older, more educated, employed, and more likely to have been married longer. Additionally, adult focused mothers reported having less rapport with their children, spent less time in joint activities with their children, and the child reported lower rapport with their mothers. Lastly, when the child and partner were resisting one another, adult focused mothers responded more to the concerns of the partner, while the child focused mothers responded more to the concerns of the child. Understanding the implications of these two differing perspectives can assist parents in their attempts to repartner.
Remarriage (Ob 17)
Rates of remarriage: Half of all marriages are remarriages for at least one partner. The rate for remarriage, like the rate for marriage, has been declining overall. In 2013 the remarriage rate was approximately 28 per 1,000 adults 18 and older. This represents a 44% decline since 1990 and a 16% decline since 2008 (Payne, 2015). Brown and Lin (2013) found that the rate of remarriage dropped more for younger adults than middle aged and older adults, and Livingston (2014) found that as we age we are more likely to have remarried (see Figure 8.33). This is not surprising as it takes some time to marry, divorce, and then find someone else to marry. However, Livingston found that unlike those younger than 55, those 55 and up are remarrying at a higher rate than in the past. In 2013, 67% of adults 55-64 and 50% of adults 65 and older had remarried, up from 55% and 34% in 1960, respectively.
Success of Remarriage: Reviews are mixed as to the happiness and success of remarriages. Cohabitation is the main way couples prepare for remarriage, but even when living together, many important issues are still not discussed. Issues concerning money, ex-spouses, children, visitation, future plans, previous difficulties in marriage, etc. can all pose problems later in the relationship. And few couples engage in premarital counseling or other structured efforts to cover this ground before entering marriage again. While some remarriages are more successful, especially if the divorce motivated the adult to engage in self-improvement and personal growth (Hetherington & Kelly, 2002), a number of divorced adults end up in very similar marriages the second or third time around (Hetherington & Kelly, 2002).
Remarriages have challenges that are not found in first marriages that may create additional stress in the marital relationship. There can often be a general lack of clarity in family roles and expectations when trying to incorporate new kin into the family structure, even determining the appropriate terms for these kin, along with their roles can be a challenge. Partners may have to navigate carefully their role when dealing with their partners’ children. All of this may lead to greater dissatisfaction and even resentment among family members. Even though remarried couples tend to have more realistic expectations for marriage, they tend to be less willing to stay in unhappy situations. The rate of divorce among remarriages is higher than among first marriages (Payne, 2015), which can add additional burdens, especially when children are involved.
Factors affecting remarriage: The chances of remarrying depend on a number of things. First, it depends on the availability of partners. As time goes by, there are more available women than men in the marriage pool. Consequently, men are more likely than women to remarry. This lack of available partners is experienced by all women, but especially by African-American women where the ratio of women to men is quite high. Women are more likely to have children living with them, and this diminishes the chance of remarriage as well. And marriage is more attractive for males than females (Seccombe & Warner, 2004). Men tend to remarry sooner (3 years after divorce on average vs. 5 years on average for women).
Many women do not remarry because they do not want to remarry. Traditionally, marriage has provided more benefits to men than to women. Women typically have to make more adjustments in work (accommodating work life to meet family demands or the approval of the husband) and at home (taking more responsibility for household duties). Further, men’s physical desirability is not as influenced by aging as is women’s. The cultural emphasis on youth and physical beauty for women does not apply for men. Today, there are more women with higher levels of education than before and women with higher levels are less likely to find partners matching this expectation. Being happily single requires being economically self-sufficient and being psychologically independent. Women in this situation may find remarriage much less attractive.
Grandparents
In addition to maintaining relationships with their children and aging parents, many people in middle adulthood take on yet another role, becoming a grandparent. In the U.S., The average age of becoming a grandparent is 50, although many individuals become grandparents even earlier (AARP, 2018). The role of grandparents varies around the world. In multigenerational households, grandparents may play a greater role in the day-to-day activities of their grandchildren. While this family dynamic is more common in Latin America, Asia, and Africa, it has been on the increase in the U.S. (Pew Research Center, 2010).
 Cherlin and Furstenberg (1986) describe three styles of grandparents:
Cherlin and Furstenberg (1986) describe three styles of grandparents:
1. Remote: Thirty percent of grandparents rarely see their grandchildren. Usually, they live far away from their grandchildren but may also have a distant relationship. Contact is typically made on special occasions, such as holidays or birthdays.
2. Companionate: Fifty-five percent of grandparents were described as “companionate.” These grandparents do things with the grandchild but have little authority or control over them. They prefer to spend time with them without interfering in parenting. They are more like friends to their grandchildren.
3. Involved: Fifteen percent of grandparents were described as “involved.” These grandparents take a very active role in their grandchild’s life. The children might even live with the grandparent. The involved grandparent is one who has frequent contact with and authority over the grandchild. Grandmothers, more so than grandfathers, play this role. In contrast, more grandfathers than grandmothers saw their role as family historian and family advisor (Neugarten & Weinstein, 1964).
Bengtson (2001) suggests that grandparents adopt different styles with different grandchildren, and over time may change styles as circumstances in the family change. Today more grandparents are the sole care providers for grandchildren or may step in at times of crisis. With these changes grandparents are redefining how they see their role in the family with fewer adopting a more formal role (Hayslip et al., 2003).
Early research on grandparents has routinely focused on grandmothers, with grandfathers often becoming invisible members of the family (Sorensen & Cooper, 2010). Yet, grandfathers stress the importance of their relationships with their grandchildren as strongly as do grandmothers (Waldrop et al., 1999). For some men, this may provide them with the opportunity to engage in activities that their occupations, as well as their generation’s views of fatherhood and masculinity kept them from engaging in with their own children (Sorenson & Cooper, 2010). Many of the grandfathers in Sorenson and Cooper’s study felt that being a grandfather was easier and a lot more enjoyable. Even among grandfathers that took on a more involved role, there was still, a greater sense that they could be more light-hearted and flexible in their interactions with their grandchildren. Many grandfathers reported that they were more openly affectionate with their grandchildren than they had been with their own children.
Productivity at Work (Ob 18)
Middle adulthood is characterized by a time of transition, change, and renewal. The midlife worker must be flexible, stay current with technology, and be capable of working within a global community. We have already discussed expertise as part of our look at cognitive development in midlife. Work and midlife include many scenarios. A person may be at their peak of performance at work during this time. Connections between work units, companies, culture, and operations may be appreciated for the first time and with that, a midlife worker may be able to contribute to an organization in new, more comprehensive ways. Midlife may also be the peak time for earning and spending to meet the demands of launching children or caring for aging parents. Some experience stable careers while others experience layoffs and find themselves back in school to gain new skills for reemployment. Others experience discrimination due to age or find it difficult to gain employment because of the higher salary demands compared with younger, less experienced workers (Barnett, 1997). In the eyes of employers, it may be more cost effective to hire a young adult, despite their limited experience, as they would be starting out at lower levels of the pay scale. In addition, hiring someone who is 25 and has many years of work ahead of them versus someone who is 55 and will likely retire in 10 years may also be part of the decision to hire a younger worker (Lachman, 2004). American workers are also competing with global markets and changes in technology. Those who are able to keep up with all these changes, or are willing to uproot and move around the country or even the world have a better chance of finding work. Some midlife adults anticipate retirement, while others may be postponing it for financial reasons.
Climate in the Workplace for Middle-aged Adults: Attitudes about work and satisfaction from work tend to undergo a transformation or reorientation during this time. Age is positively related to job satisfaction—the older we get the more we derive satisfaction from work (Ng & Feldman, 2010). A number of studies have found that job satisfaction tends to peak in middle adulthood (Besen et al., 2013; Easterlin, 2006). This satisfaction stems from not only higher wages, but often greater involvement in decisions that affect the workplace as they move from worker to supervisor or manager. Job satisfaction is also influenced by being able to do the job well, and after years of experience at a job, many people are more effective and productive. Another reason for this peak in job satisfaction is that at midlife many adults lower their expectations and goals (Tangri et al., 2003). Middle-aged employees may realize they have reached the highest they are likely to in their career. This satisfaction at work translates into lower absenteeism, greater productivity, and less job hopping in comparison to younger adults (Easterlin, 2006).
However, not all middle-aged adults are happy in the workplace. Dobrow et al. (2018) found that job satisfaction in those aged 43-51 was correlated with advancing age, but that there was increased dissatisfaction the longer one stayed in the same job. There is a reluctance to tolerate a work situation deemed unsuitable or unsatisfying. Years left, as opposed to years spent, necessitates a sense of purpose in all daily activities and interactions, including work. Additionally, women may find themselves up against the glass ceiling, organizational discrimination in the workplace that limits the career advancement of women. This may explain why females employed at large corporations are twice as likely to quit their jobs as are men (Barreto et al., 2009). Another problem older workers may encounter is job burnout, becoming disillusioned and frustrated at work. American workers may experience more burnout than do workers in many other developed nations because most developed nations guarantee by law a set number of paid vacation days (International Labour Organization, 2011), the United States does not (U.S. Department of Labor, 2016). Not all employees are covered under overtime pay laws (U.S. Department of Labor, 2016). This is important when you considered that the 40-hour work week is a myth for most Americans. Only 4 in 10 U.S. workers work the typical 40- hour work week. The average workweek for many is almost a full day longer (47 hours), with 39% working 50 or more hours per week (Saad, 2014). In comparison to workers in many other developed nations, American workers work more hours per year (Organisation for Economic Cooperation and Development, 2016). Americans work more hours than most European nations, especially western and northern Europe, although they work fewer hours than workers in other nations, especially Mexico.
One of the most influential researchers in this field, Dorien Kooij (2013) identified four key motivations in older adults continuing to work. First, growth or development motivation- looking for new challenges in the work environment. The second are feelings of recognition and power. Third, feelings of power and security afforded by income and possible health benefits. Interestingly enough, the fourth area of motivation was Erikson’s generativity. The latter has been criticized for a lack of support in terms of empirical research findings, but two studies (Zacher et al, 2012; Ghislieri & Gatti, 2012) found that a primary motivation in continuing to work was the desire to pass on skills and experience, a process they describe as leader generativity. Perhaps a more straightforward term might be mentoring. In any case, the concept of generative leadership is now firmly established in the business and organizational management literature.

The workplace today is one in which many people from various walks of life come together. Work schedules are more flexible and varied, and more work independently from home or anywhere there is an internet connection. The midlife worker must be flexible, stay current with technology, and be capable of working within a global community. And the midlife mind seeks meaningful work.
Reflection activity: Preparing for Middle Age
“Aging is the extraordinary process whereby you become the person you always should have been.” —David Bowie
Visualize your possible self as a fifty-five-year-old adult self. If you are already fifty-five years old or older, then compare what you would have imagined as a twenty-two-year-old with your actual self. What is your life like at fifty-five years old? What are the most important relationships in your life? Where are you living? What makes you happy? What have been your biggest challenges? Use that visualization to chart a pathway from early adulthood through middle adulthood that focuses on one or two important goals for well-being that utilize your current strengths and priorities to address challenges and maximize healthy and productive growth.
- Two important goals as I complete middle adulthood are (1)________(2)__________
- How do these goals align with my current priorities and values? _________________
- What strengths do I already have that will help me to reach these goals? (1)___ (2)___
- What challenges do I anticipate in trying to reach these goals (could be personal, environmental, or social factors)? (1)________________ (2)_______________________
- What resources will I need to find or develop to help address these challenges (could be personal, environmental, or social factors)? (1)____________ (2)_______________
- What are the next best steps towards achieving this goal? (1)__________ (2) _______
- How will my life change once I achieve this goal? What will improve? What new challenges might arise? ___________________________________________________
Conclusion
We have portrayed midlife as a central, pivotal period in the life course. Midlife is a period of transition. This is a pivotal period in the life course in terms of balancing growth and decline, linking earlier and later periods of life, and bridging younger and older generations. Midlife links childhood experiences with midlife health and lifestyle in midlife with health in old age. Overall, longitudinal research indicates that overall perceptions of well being and life satisfaction tend to increase in middle adulthood (Buecker et al., 2023). Middle adulthood also plays out at the interpersonal, intergenerational levels through roles such as parenting, caregiving, and mentoring. It is also a time of productivity and expertise; a time of putting things together. A clear sense of self, identity, and control can be important for meeting the challenges of midlife (Lachman & Firth, 2004). We understand more about midlife in the context of the life course. Yet, there is more to be learned. The story of midlife will continue to unfold as more attention is given to it as a part of the lifespan.
Chapter Review Practice Quiz
Chapter 10 Key terms (see Glossary)
|
4-horsemen (Gottman)
|
hypertension |
| andropause | kinkeeping |
|
big-5 personality traits
|
menopause |
| boomerang kids | novice |
|
crystallized intelligence
|
overload stressors
|
| diabetes | plasticity |
|
emotion-focused coping
|
presbyopia |
| empty nest |
problem-focused coping
|
| expertise |
rheumatoid arthritis
|
| flow | sarcopenia |
| fluid intelligence | sleep apnea |
| gallstones | stress |
|
gender dysphoria
|
sudden cardiac arrest
|
|
generativity vs. stagnation (Erikson)
|
tacit knowledge |
| goodness-of-fit | |
| heart disease | |
| heartburn |
Media Attributions
- pexels-kindelmedia-7938727 © Kindel Media is licensed under a CC0 (Creative Commons Zero) license
- 03 © pixabay is licensed under a CC BY (Attribution) license
- Chapter_10_Middle_Adulthood_Include_V3_01 © pixabay is licensed under a CC BY (Attribution) license
- OSX_Lifespan_13_02_HeartSigns
- Private: Chapter_10_Middle_Adulthood_Include_V3_02 © Wikimedia is licensed under a CC BY (Attribution) license
- Chapter_10_Middle_Adulthood_Include_V3_03 © National Institute of Diabetes and Digestive and Kidney Diseases is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_10_Middle_Adulthood_Include_V3_04 © Wikimedia is licensed under a CC BY-SA (Attribution ShareAlike) license
- 04 © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- 05 © mollybee is licensed under a CC BY-SA (Attribution ShareAlike) license
- pexels-timur-weber-8560801 is licensed under a CC BY (Attribution) license
- pexels-karolina-grabowska-6028521 © Kaboompics is licensed under a CC0 (Creative Commons Zero) license
- Yoga Position © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_9_Early_Adulthood_Include_V3_09 is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_9_Early_Adulthood_Include_V3_10 © Wikimedia is licensed under a CC BY-SA (Attribution ShareAlike) license
- car-coat-vehicle-auto-black-sports-car-719158-pxhere.com is licensed under a Public Domain license
- 09 © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- Lady on Phone © Pxhere is licensed under a CC BY-SA (Attribution ShareAlike) license
- 11 © Pixabay
- pexels-gary-barnes-6248806 © Gary Barnes is licensed under a CC0 (Creative Commons Zero) license
- pexels-transtudios-13456845 is licensed under a CC0 (Creative Commons Zero) license
- 800px-Nukus_-_Khiva,_near_Qyzyl_Qala_(6226941430) is licensed under a CC BY-SA (Attribution ShareAlike) license
- pexels-olly-3863783 © Andrea Piacquadio is licensed under a CC0 (Creative Commons Zero) license
farsightedness caused by loss of elasticity of the lens of the eye, occurring typically in middle and old age
reduction in skeletal muscle mass due to aging
refers to several types of heart conditions including coronary artery disease (CAD). High blood pressure, high blood cholesterol, and smoking are key risk factors
unexpected loss of heart functioning, breathing, and consciousness
high blood pressure
a variable disorder of carbohydrate metabolism caused by a combination of hereditary and environmental factors and usually characterized by inadequate secretion or utilization of insulin, by excessive urine production, by excessive amounts of sugar in the blood and urine, and by thirst, hunger, and loss of weight – Diabetes Mellitus
a usually chronic autoimmune disease that is characterized especially by pain, stiffness, inflammation, swelling, and sometimes destruction of joints
a burning discomfort behind the lower part of the sternum due especially to spasmodic reflux of acid from the stomach into the esophagus
a burning discomfort behind the lower part of the sternum due especially to spasmodic reflux of acid from the stomach into the esophagus
the natural cessation of menstruation that usually occurs between the ages of 45 and 55
collection of symptoms, including fatigue and a decrease in libido, experienced by some middle-aged or older men and attributed to a gradual decline in testosterone levels
sleeping disorder in which the temporary cessation of breathing occurs more often than normal during sleep, and can cause hypoxemia and sleep deprivation
one of bodily or mental tension resulting from factors that tend to alter an existent equilibrium
to apply coping skills directly to the source of a distressing situation. Purpose to combat stress directly
using skills for processing and dealing with feelings that arise due to stressful situations. It utilizes inward-facing strategies
pragmatic or practical and learned through experience rather than explicitly taught
intelligence can be shaped by experience
refers to the capacity to learn new ways of solving problems and performing activities quickly and abstractly
refers to the accumulated knowledge of the world, we have acquired throughout our lives
the mental state of being completely present and fully absorbed in a task
refers to specialized skills and knowledge that pertain to a particular topic or activity
someone who has limited experiences with a particular task
a distressed state arising from conflict between a person’s gender identity and the sex the person has or was identified as having at birth
stage of Erikson theory, midlife adults time period to strive to create or nurture things that will outlast them, often by parenting children or fostering positive changes that benefit others (generative) vs no doing so and feeling stagnation
openness, conscientiousness, extraversion, agreeableness, neuroticism
parent style match and communication and interaction can flow - understanding child dimension of temperament
having too many demands placed on them by children or do to financial concerns
the seemingly empty home after the parents’ children have left the house indefinitely
a young adult who returns to live at his or her family home especially for financial reasons
organizing events and communication in order to maintain family ties
Gottman's 4-horsemen that can harm relationships (marriages): contempt, criticism, defensiveness, and stonewalling
