
Chapter 5: Early Childhood

Objectives:
At the end of this chapter, you will be able to…
- Summarize overall physical growth during early childhood. Identify examples of gross and fine motor skill development in early childhood.
- Describe growth of structures in the brain during early childhood.
- Identify nutritional concerns for children in early childhood.
- Describe sexual development in early childhood. Define preoperational intelligence.
- Identify animism, egocentrism, and centration.
- Describe changes to attention and memory in early childhood.
- Apply Vygotsky theory to early childhood. Illustrate scaffolding. Explain private speech. Explain theory of mind.
- Describe language development in early childhood.
- Explain Erikson’s stages of psychosocial development for toddlers and children in early childhood.
- Contrast models of parenting styles.
- Examine concerns about child care.
- Explain theory of self from Mead.
- Summarize theories of gender role development.
- Examine concerns about childhood stress and development.
The objectives are associated with the reading sections below.
Introduction
Our discussion will now focus on the physical, cognitive and socioemotional development during the ages from two to six, referred to as early childhood. Early childhood represents a time period of continued rapid growth, especially in the areas of language and cognitive development. Those in early childhood have more control over their emotions and begin to pursue a variety of activities that reflect their personal interests. Parents continue to be very important in the child’s development, but now teachers and peers exert an influence not seen with infants and toddlers.
Physical Development during Early Childhood
Growth in early childhood (Ob 1)
Children between the ages of 2 and 6 years tend to grow about 3 inches in height each year and gain about 4 to 5 pounds in weight each year. The 3-year-old is very similar to a toddler with a large head, large stomach, short arms, and legs. During early childhood, children start to lose some of their baby fat, making them less like a baby, and more like a child as they progress through this stage. By around age 3, children will have all 20 of their primary teeth, and by around age 4, may have 20/20 vision. But by the time the child reaches age 6, the torso has lengthened and body proportions have become more like those of adults. At six years of age, the average child in the United States is 45 inches tall (approximately 115 cm) and weighs 45 pounds (approximately 20.4 kg) (Centers for Disease Control and Prevention [CDC], 2023).
Evidence indicates that the full height potential of our genetic inheritance is affected by several environmental influences. Economic disadvantage, physical neglect, disease, and malnutrition can affect biological and epigenetic mechanisms associated with height, which can take several generations to return to the normal range (Bogin, 2013; Lang et al., 2019; Simeone & Alberti, 2014). These influences may partly explain generational variations in height.
This growth rate is slower than that of infancy and is accompanied by a reduced appetite between the ages of 2 and 6. This change can sometimes be surprising to parents and lead to the development of poor eating habits. What children are eating is important to consider. Children who consume a lot of high-fat, sweet, and salty foods may fail to acquire a taste for other flavors. In contrast, adults who model positive eating habits, gently encourage children to try new foods, and avoid arguments over meals have a positive impact on children’s eating behavior. In short, children who are introduced to healthy vegetables and proteins on a regular basis will grow accustomed to them (Cardona Cano et al., 2015; Mahmood et al., 2021; Mazza et al., 2022; Nekitsing et al., 2018). Children between the ages of 2 and 3 need 1,000 to 1,400 calories, while children between the ages of 4 and 8 need 1,200 to 2,000 calories (Mayo Clinic, 2016a).
Nutritional concerns (Ob 3)
One directly observable consequence of malnutrition is stunting, or impaired growth in height. Stunting, which cannot be reversed and can increase cognitive and physical damage risks, has become a global concern (De Sanctis et al., 2021; Bhutta et al., 2020). Particularly in war-torn, severely impoverished, and drought-stricken areas, inadequate nutrition is widespread, and stunting is an inherent risk. As a result, an estimated 149 million children under five, or more than 20 percent of the global under-five population, undergo stunting. In some poor parts of Africa and southern Asia, the proportion rises to nearly half (UNICEF/World Health Organization [WHO]/World Bank Group, 2021).
Malnutrition is not common in developed nations like the United States, yet many children lack a balanced diet. Added sugars and solid fats contribute to 40% of daily calories for children and teens in the US. Approximately half of these empty calories come from six sources: soda, fruit drinks, dairy desserts, grain desserts, pizza, and whole milk (CDC, 2015). Caregivers need to keep in mind that they are setting up taste preferences at this age. Young children who grow accustomed to a high fat, very sweet, and salty flavors may have trouble eating foods that have subtler flavors such as fruits and vegetables.

By providing adequate, sound nutrition, and limiting sugary snacks and drinks, the caregiver can be assured that 1) the child will not starve, and 2) the child will receive adequate nutrition. Preschoolers can experience iron deficiencies if not given well-balanced nutrition and if given too much milk. Calcium interferes with the absorption of iron in the diet as well.
Consider the following advice about establishing eating patterns for years to come (Rice, 1997). Notice that keeping mealtime pleasant, providing sound nutrition, and not engaging in power struggles over food are the main goals:
Tips for Establishing Healthy Eating Patterns
| Don’t try to force your child to eat or fight over food. Of course, it is impossible to force someone to eat. But the real advice here is to avoid turning food into some kind of ammunition during a fight. Do not teach your child to eat to or refuse to eat in order to gain favor or express anger toward someone else. Recognize that appetite varies. Children may eat well at one meal and have no appetite at another. Rather than seeing this as a problem, it may help to realize that appetites do vary. Continue to provide good nutrition, but do not worry excessively if the child does not eat. Keep it pleasant. This tip is designed to help caregivers create a positive atmosphere during mealtime. Meal times should not be the time for arguments or expressing tensions. You do not want the child to have painful memories of mealtimes together or have nervous stomachs and problems eating and digesting food due to stress. No short order chefs. While it is fine to prepare foods that children enjoy, preparing a different meal for each child or family member sets up an unrealistic expectation from others. Children probably do best when they are hungry and a meal is ready. Limiting snacks rather than allowing children to “graze” continuously can help create an appetite for whatever is being served. Limit choices. If you give your preschool-aged child choices, make sure that you give them one or two specific choices rather than asking “What would you like for lunch?” If given an open choice, children may change their minds or choose whatever their sibling does not choose! Serve balanced meals. This tip encourages caregivers to serve balanced meals. A box of macaroni and cheese is not a balanced meal. Meals prepared at home tend to have better nutritional value than fast food or frozen dinners. Prepared foods tend to be higher in fat and sugar content as these ingredients enhance taste and profit margin because fresh food is often costlier and less profitable. However, preparing fresh food at home is not costly. It does, however, require more activity. Preparing meals and including the children in kitchen chores can provide a fun and memorable experience. Don’t bribe. Bribing a child to eat vegetable by promising desert is not a good idea. For one reason, the child will likely find a way to get the desert without eating the vegetables (by whining or fidgeting, perhaps, until the caregiver gives in), and for another reason, because it teaches the child that some foods are better than others. Children tend to naturally enjoy a variety of foods until they are taught that some are considered less desirable than others. A child, for example, may learn the broccoli they have enjoyed is seen as yucky by others unless it’s smothered in cheese sauce! |

To what extent do these tips address cultural practices? How might these tips vary by culture?
Brain Maturation (Ob 2)
Brain weight: If you recall, the brain is about 75 percent of its adult weight by two years of age. By age 6, it is at 95 percent its adult weight (yet only 30 percent of an adult body weight). Myelination and the development of dendrites continue to occur in the cortex and as it does, we see a corresponding change in what the child is capable of doing. The myelination of neurons that are essential to early physical development is mostly complete by 40 months of age. However, when life experiences are limited or the environment is highly stressful, myelination and overall brain growth will be slowed.
From an early age, the amount of stimulation a child receives has a significant effect on brain structure, weight, and volume (Gilmore et al, 2018; Lawson, 2013; Ziegler et al., 2020). Poor nutrition may also lead to deficits in myelin development and a general decrease in brain mass. However, the brain remains quite plastic in early childhood, and early intervention can often reverse these negative effects (de Faria et al., 2019). The brain continues to overproduce dendrites and synapses, which then leads to additional synaptic pruning. This alone tells us that brain plasticity remains strong, and that experiences and opportunities have roles in development. That the brain continually reorganizes itself tells us that a person’s environment has a persistent influence on outcomes.
Greater development in the prefrontal cortex, the area of the brain behind the forehead that helps us to think, strategizes, and controls emotion, makes it increasingly possible to control emotional outbursts and to understand how to play games. The process of overproduction and pruning of synapses probably doesn’t stop until the third decade of life, especially in the prefrontal cortex (Kolk & Rakic, 2022).
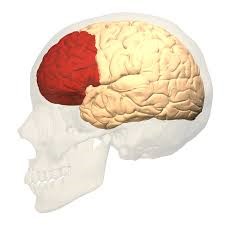
Consider 4 or 5-year-old children and how they might approach a game of soccer. Chances are every move would be a response to the commands of a coach standing nearby calling out, “Run this way! Now, stop. Look at the ball. Kick the ball!” And when the child is not being told what to do, he or she is likely to be looking at the clover on the ground or a dog on the other side of the fence! Understanding the game, thinking ahead, and coordinating movement improves with practice and myelination. Not being too upset over a loss, hopefully, does as well.
Growth in the Hemispheres and Corpus Callosum: The brain is lateralized. this organizational characteristic of the brain is known as lateralization. The left hemisphere typically handles language-related tasks such as reading, speaking, and thinking, while the right hemisphere specializes in emotional expression, musical ability, and recognition of visual-spatial relationships used in geometry, art, and navigation. Between ages 3 and 6, the left hemisphere of the brain grows dramatically. The right hemisphere continues to grow throughout early childhood and is involved in tasks that require spatial skills, such as recognizing shapes and patterns. The corpus callosum, a dense band of fibers that connects the two hemispheres of the brain, contains approximately 200 million nerve fibers that connect the hemispheres (Kolb & Whishaw, 2011).
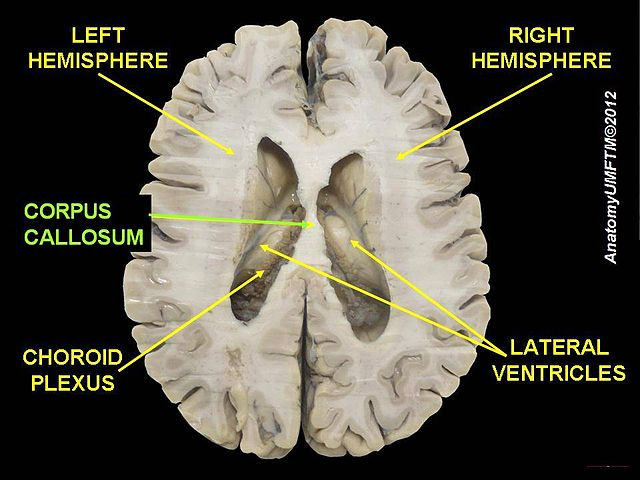
The corpus callosum is located a couple of inches below the longitudinal fissure, which runs the length of the brain and separates the two cerebral hemispheres (Garrett, 2015). The hemispheres are independent, and they work together to process experiences and respond from the corpus callosum. Because the two hemispheres communicate with each other and integrate their activities through the corpus callosum. Additionally, because incoming information is directed toward one hemisphere, such as visual information from the left eye being directed to the right hemisphere, the corpus callosum shares this information with the other hemisphere. For example, reading a word relies on the right-hemisphere functions for visualization and then oral communication is a function of the left hemisphere. (There is no such thing as being “left-brained” or “right-brained.”)
The corpus callosum undergoes a growth spurt between ages 3 and 6, and this results in improved coordination between right and left hemisphere tasks. For example, in comparison to other individuals, children younger than 6 demonstrate difficulty coordinating an Etch A Sketch toy because their corpus callosum is not developed enough to integrate the movements of both hands (Kalat, 2016).
Neuroplasticity: The control of some specific bodily functions, such as movement, vision, and hearing, is performed in specified areas of the cortex, and if these areas are damaged, the individual will likely lose the ability to perform the corresponding function. For instance, if an infant suffers damage to facial recognition areas in the temporal lobe, it is likely that he or she will never be able to recognize faces (Farah et al., 2000). On the other hand, the brain is not divided up in an entirely rigid way. The brain’s neurons have a remarkable capacity to reorganize and extend themselves to carry out particular functions in response to the needs of the organism, and to repair the damage. As a result, the brain constantly creates new neural communication routes and rewires existing ones. Neuroplasticity refers to the brain’s ability to change its structure and function in response to experience or damage. Neuroplasticity enables us to learn and remember new things and adjust to new experiences. Our brains are the most “plastic” when we are young children, as it is during this time that we learn the most about our environment. On the other hand, neuroplasticity continues to be observed even in adults (Kolb & Fantie, 1989).
Right or left-handed?
Handedness is an example of lateralization in action. About 10 percent of children across cultures and continents prefer to use their left hand, a preference linked to differences in brain organization and genes. Whereas about 95 percent of right-handed people show typical lateralization patterns (like language centers in the left hemisphere), only about 75 percent of left-handers do (de Kovel et al., 2019). Though some studies indicate that most children develop an obvious hand preference by six months of age, others find that stable preferences may not appear until age nine or even later (Scharoun & Bryden, 2014). However, by that time, most children have already been required to favor one hand over another in school tasks like coloring, writing, and using a mouse.
Differences in cognition, artistic expression, and athletic prowess between left-handed and right-handed children are often reported. However, no scientific evidence suggests that these differences exist (McManus, 2019). Nonetheless, children who are left-hand dominant often struggle with products designed for right-handers, such as scissors, seat belts, and school desks. Though we can learn to use our non-dominant hand quite well, hand dominance appears to be highly heritable and unchangeable. Even identical twins, who share the same genes, may favor different hands; each has the same 10 percent chance of being left-handed. This indicates that handedness results from a combination of environmental and genetic influences (Schmitz et al., 2017).
Motor Skill Development (Ob 1)

Early childhood is a time when children are especially attracted to motion and song. Days are filled with moving, jumping, running, swinging, and clapping and every place becomes a playground. Even the booth at a restaurant affords the opportunity to slide around in the seat or disappear underneath and imagine being a sea creature in a cave! Of course, this can be frustrating to a caregiver, but it’s the business of early childhood. Children continue to improve their gross motor skills as they run and jump, and frequently ask their caregivers to “look at me” while they hop or roll down a hill. Gross motor skills involve larger muscle groups in legs and arms or entire body. Children’s songs are often accompanied by arm and leg movements or cues to turn around or move from left to right. Fine motor skills involve smaller action muscle coordination, and are also being refined in activities such as pouring water into a container, drawing, coloring, and using scissors. Some children’s songs promote fine motor skills (have you ever heard of the song “itsy, bitsy, spider”?).

The development of greater coordination of muscles groups and finer precision can be seen during this time period. Thus, average 2-year-olds may be able to run with slightly better coordination than they managed as a toddler, yet they would have difficulty pedaling a tricycle, something the typical 3-year-old can do. We see similar changes in fine motor skills with 4-year-olds who no longer struggle to put on their clothes, something they may have had problems with two years earlier. Mastering the fine art of cutting one’s own fingernails or tying shoes will take a lot of practice and maturation. Motor skills continue to develop into middle childhood, but for those in early childhood, play that deliberately involves these skills is emphasized.
By the time children arrive at middle childhood, they will have developed the general capabilities to perform movements like those of adults—though with far less skill and strength. However, due to their relatively immature cognitive abilities and still-developing brains, children don’t yet fully grasp certain aspects of motion, such as the trajectory of a rolling ball in a game of soccer or kickball. For these reasons, younger children are usually offered accommodations when engaging in physical activities. For instance, their slower reaction time and lack of skill necessitates the use of equipment like training wheels on a bicycle or a batting tee in T-ball.
Table: Examples of Motor skill Milestones for children 2 to 5 years old
| Gross Motor Skills | Fine Motor Skills | |
| Age 2 |
Can kick a ball without losing balance Can pick up objects while standing, without losing balance (This often occurs by 15 months. It is a cause for concern if not seen by 2 years.) Can run with better coordination. (May still have a wide stance.) |
Able to turn a doorknob Can look through a book turning one page at a time Can build a tower of six to seven cubes Able to put on simple clothes without help (The child is often better at removing clothes than putting them on) |
| Age 3 |
Can briefly balance and hop on one foot May walk on stairs with alternating feet (without holding onto rail) Can pedal a tricycle |
Can build a block tower of more than nine cubes Can easily place small objects in a small opening Can copy a circle Drawing a person with 3 parts Feeds self easily |
| Age 4 |
Shows improved balance Hops on one foot without losing balance Throws a ball overhead with coordination |
Can cut out a picture using scissors Drawing a square Managing a spoon and fork neatly while eating Putting on clothes properly |
| Age 5 |
Has better coordination (getting the arms, legs, and body to work together) Skips, jumps and hops with good balance Stays balanced while standing on one foot with eyes closed |
Shows more skills with simple tools and writing utensils Can copy a triangle Can use a knife to spread soft foods |
Table adapted from (NIH, 2018)
Children’s art: Have you ever examined the drawings of young children? If you look closely, you can almost see the development of motor skills, perceptual understanding, and cognition reflected in the way these images change as pathways become more mature. Early scribbles and dots illustrate the use of simple motor skills. No real connection is made between an image being visualized and what is created on paper.
Rhoda Kellogg (1969) noted that children’s drawings underwent several transformations. Starting with about 20 different types of scribbles at age 2, children move on to experimenting with the placement of scribbles on the page. By age 3 they are using the basic structure of scribbles to create shapes and are beginning to combine these shapes to create more complex images. By 4 or 5 children are creating images that are more recognizable representations of the world. These changes are a function of improvement in motor skills, perceptual development, and cognitive understanding of the world (Cote & Golbeck, 2007).
The drawing of tadpoles is a pervasive feature of young children’s drawings of self and others. Tadpoles emerge in children’s drawing at about the age of 3 and have been observed in the drawings of young children around the world (Gernhardt et al., 2015). Despite the universality of tadpoles in children’s drawings, there are cultural variations in the size, number of facial features, and emotional expressions displayed. Gernhardt et al. (2015) found that children from Western contexts (i.e., urban areas of Germany and Sweden) and urban educated non-Western contexts (i.e., urban areas of Turkey, Costa Rica, and Estonia) drew larger images, with more facial detail and more positive emotional expressions, while those from non-Western rural contexts (i.e., rural areas of Cameroon and India) depicted themselves as smaller, with less facial details and a more neutral emotional expression. The authors suggest that cultural norms of non-Western traditionally rural cultures, which emphasize the social group rather than the individual, may be one of the factors for the difference in the size of the figure. The tadpole figures of children from Western cultures often took up most of the page. Coming from cultures that emphasize the individual, this should not be surprising.
Physical Activity is Important!
We know that during early childhood, parents and caregivers should encourage activities and play that emphasize motor skills and combat sedentary behavior and habits. After all, the brain literally grows when children engage in new opportunities. Additionally, it’s well-established that early physical activity has a positive impact on later health outcomes (Pate et al., 2019; Roychowdhury, 2020; Wyszyńska et al., 2020), including weight and cardiovascular fitness. It is also linked to lower risks of chronic diseases like diabetes, hypertension, and certain cancers. Moreover, children who engage in physical activity during early childhood have higher bone density, which may help prevent osteoporosis in later life (Pate et al., 2019).
Active children also have stronger cognitive development, including improved attention, self-regulation, and academic performance (Mualem et al., 2018; Wood et al., 2020). Substantial evidence shows that throughout the lifespan, regular physical activity leads to better overall cognitive development (Erickson et al., 2019). Even a single 30-minute session has been shown to be beneficial in improving motor activity and memory for preschool children (McDonnell et al., 2013).
Here are the recommendations from WHO (2024):
- three- and four-year-old children should spend a minimum of three hours per day engaged in a variety of physical activities, including at least sixty minutes of moderate intensity to promote overall healthy development (WHO, 2022). Moderately intense activities include walking a dog, dancing, and riding a tricycle.
- five to six years old, the WHO recommends that children participate in a minimum of sixty minutes of moderate-to-vigorous activity per day. This can include normal school recess activities like climbing and playing games with balls. At least three times per week, children this age should engage in more vigorous aerobic activity, like games of tag, soccer, or basketball. High-intensity physical activities are especially important for building bone strength and muscle development (Gunter et al., 2012; Specker et al., 2015).
Get kids to get moving!
Toilet Training

Toilet training typically occurs during the first two years of early childhood (24-36 months). Some children show interest by age 2, but others may not be ready until months later. The average age for girls to be toilet trained is 29 months and for boys, it is 31 months (Boyse & Fitzgerald, 2010). One study indicated that only 40 to 60 percent of children complete toilet training by 36 months of age (Blum et al., 2004). Most children have control over both bladder and bowels and leave diapers behind sometime between 3 and 4 years old. The child’s age is not as important as his/her physical and emotional readiness. If started too early, it might take longer to train a child.
According to the Mayo Clinic (2016b), the following questions can help parents determine if a child is ready for toilet training:
- Does your child seem interested in the potty chair or toilet, or in wearing underwear?
- Can your child understand and follow basic directions?
- Does your child tell you through words, facial expressions or posture when he or she needs to go?
- Does your child stay dry for periods of two hours or longer during the day?
- Does your child complain about wet or dirty diapers?
- Can your child pull down his or her pants and pull them up again?
- Can your child sit on and rise from a potty chair? (p. 1)
If a child resists being trained or it is not successful after a few weeks, it is best to take a break and try again later. Most children master daytime bladder control first, typically within two to three months of consistent toilet training. However, nap and nighttime training might take months or even years.
Some children experience elimination disorders that may require intervention by the child’s pediatrician or a trained mental health practitioner. Elimination disorders include enuresis, or the repeated voiding of urine into bed or clothes (involuntary or intentional) and encopresis, the repeated passage of feces into inappropriate places (involuntary or intentional) (American Psychiatric Association, 2013). The prevalence of enuresis is 5%-10% for 5-year-olds, 3%-5% for 10-year-olds and approximately 1% for those 15 years of age or older. Around 1% of 5-year-olds have encopresis, and it is more common in males than females.
Sleep

Sleep is important for mood regulation and attention (NSF, 2015). In cases where children are tired they actually do not look tired. Children needing more sleep may resist bedtime and become hyper as the evening goes on. During early childhood, there is wide variation in the number of hours of sleep recommended per day. For example, 2-year-olds may still need 14 hours per day, while a six-year-old may only need 9 hours. According to the WHO, preschool children typically need ten to thirteen hours of sleep every twenty-four hours and to maintain consistent sleep and wake times. Children who have stopped napping sleep more at night, getting the same amount of sleep overall as their peers who nap (Ward et al., 2008; WHO, 2019).
The National Sleep Foundation’s 2015 recommendations based on age are listed in the next table.
Table. Age groups and sleep duration recommendations
| Age Range | Typically needed each day | May be appropriate |
| Infant (4-11 months) | 12-15 hours | Not less than 10 and not more than 18 hours |
| Toddler (1-2 years) | 11-14 hours | Not less than 9 and not more than 16 hours |
| Preschooler (3-5 years) | 10-13 hours | Not less than 8 and not more than 14 hours |
| School age (6-13 years) | 9-11 hours | Not less than 7 and not more than 12 hours |
| Teenager (14-17 years) | 8-10 hours | Not less than 7 and not more than 11 hours |
Table adapted from Hirskowitz (2015)
Sexual Development in Early Childhood (Ob 4)
Sexual and gender development are two different processes, but a misconception is that they are connected. We will first focus on children’s sexual development, and later in the chapter discuss gender development. Historically, children have been thought of as innocent or incapable of sexual arousal (Aries, 1962). Yet, the physical dimension of sexual arousal is present from birth. However, it is not appropriate to associate the elements of seduction, power, love, or lust that is part of the adult meanings of sexuality. Sexuality begins in childhood as a response to physical states and sensation and cannot be interpreted as similar to that of adults in any way (Carroll, 2007).
Boys and girls are capable of erections and vaginal lubrication even before birth (Martinson, 1981). Arousal can signal overall physical contentment and stimulation that accompanies feeding or warmth. And infants begin to explore their bodies and touch their genitals as soon as they have sufficient motor skills. This stimulation is for comfort or to relieve tension rather than to reach orgasm (Carroll, 2007).
Early Childhood: Children 4 years old and younger are naturally immodest, and may display open—and occasionally startling–curiosity about other people’s bodies and bodily functions, such as touching women’s breasts, or wanting to watch when grownups go to the bathroom (NCTSN, 2009). Wanting to be naked (even if others are not) and showing or touching private parts while in public are also common in young children (NCTSN, 2009). They are curious about their own bodies and may quickly discover that touching certain body parts feels nice (NCTSN, 2009). Self-stimulation is common in early childhood for both boys and girls. Curiosity about the body and about others’ bodies is a natural part of early childhood as well.
As children age and interact more with other children (approximately ages 4–6), they become more aware of the differences between boys and girls, and more social in their exploration (NCTSN, 2009). As children grow, they are more likely to show their genitals to siblings or peers, and to take off their clothes and touch each other (Okami et al., 1997). In addition to exploring their own bodies through touching or rubbing their private parts (masturbation), they may begin “playing doctor” and copying adult behaviors such as kissing and holding hands (NCTSN, 2009). Boys are often shown by other boys how to masturbate. Boys masturbate more often and touch themselves more openly than do girls (Schwartz, 1999). As children become increasingly aware of the social rules governing sexual behavior and language (such as the importance of modesty or which words are considered “naughty”), they may try to test these rules by using naughty words (NCTSN, 2009). They may also ask more questions about sexual matters, such as where babies come from, and why boys and girls are physically different (NCTSN, 2009). Messages about what is going on and the appropriate time and place for such activities help the child learn what is appropriate.
What is typical for young children’s sexuality? (NCTSN, 2009)
| Preschool children (less than 4 years) ■ Explore and touch private parts, in public and in private ■ Rub private parts (with hand or against objects) ■ Show private parts to others ■ Try to touch mother’s or other women’s breasts ■ Remove clothes and wanting to be naked ■ Attempt to see other people when they are naked or undressing (such as in the bathroom) ■ Ask questions about their own—and others’—bodies and bodily functions ■ Talking to children their own age about bodily functions such as “poop” and “pee” |
| Young Children (approximately 4-6 years) ■ Purposefully touch private parts (masturbation), occasionally in the presence of others ■ Attempt to see other people when they are naked or undressing ■ Mimic dating behavior (such as kissing, or holding hands) ■ Talk about private parts and using “naughty” words, even when they don’t understand the meaning ■ Explore private parts with children |
Parents play a pivotal role in helping their children develop healthy attitudes and behaviors towards sexuality (NCTSN, 2009). Although talking with your children about sex may feel outside your comfort zone, there are many resources available to help you begin and continue the conversation about sexuality. It is important to remain calm and event tone and ask open-ended questions when you feel unsettled over something your child said or you have seen him/her do. A behavior that is not typical should not be ignored and it may mean that your child needs to learn something from the situation (e.g., private parts are private). Providing close supervision, and providing clear, positive messages about modesty, boundaries, and privacy are crucial as children move through the periods of childhood (NCTSN, 2009). By talking openly with your children about relationships, intimacy, and sexuality, you can foster their healthy growth and development (NCTSN, 2009).
Basic Information Parents can share with Early Childhood (Before 4 years old) (NCTSN, 2009)
| ■ Boys and girls are different ■ Accurate names for body parts of boys and girls ■ Babies come from mommies ■ Rules about personal boundaries (for example, keeping private parts covered, not touching other children’s private parts) ■ Give simple answers to all questions about the body and bodily functions. |

Photo courtesy of Flickr |
Safety Information for Early Childhood (NCTSN, 2009)
■ The difference between “okay” touches (which are comforting, pleasant, and welcome) and “not okay” touches (which are intrusive, uncomfortable, unwanted, or painful)
■ Your body belongs to you
■ Everyone has the right to say “no” to being touched, even by grown-ups
■ No one—child or adult–has the right to touch your private parts
■ It’s okay to say “no” when grownups ask you to do things that are wrong, such as touching private parts or keeping secrets from mommy or daddy
■ There is a difference between a “surprise”–which is something that will be revealed sometime soon, like a present—and a “secret,” which is something you’re never supposed to tell. Stress that it is never okay to keep secrets from mommy and daddy
■ Who to tell if people do “not okay” things to you, or ask you to do “not okay” things to them
Basic Information to share with Young Children (approximately 4-6 years) (NCTSN, 2009)
| ■ Boys’ and girls’ bodies change when they get older. ■ Simple explanations of how babies grow in their mothers’ wombs and about the birth process. ■ Rules about personal boundaries (such as, keeping private parts covered, not touching other children’s private parts) ■ Simple answers to all questions about the body and bodily functions ■ Touching your own private parts can feel nice, but is something done in private |

Photo courtesy of Flickr |
Safety Information for Young Children (NCTSN, 2009)
■ Sexual abuse is when someone touches your private parts or asks you to touch their private parts
■ It is sexual abuse even if it is by someone you know
■ Sexual abuse is NEVER the child’s fault
■ If a stranger tries to get you to go with him or her, run and tell a parent, teacher, neighbor, police officer, or other trusted adult
■ Who to tell if people do “not okay” things to you, or ask you to do “not okay” things to them (NCTSN, 2009)
Cognitive Development
Early childhood is a time of pretending, blending fact and fiction, and learning to think of the world using language. As young children move away from needing to touch, feel, and hear about the world toward learning some basic principles about how the world works, they hold some pretty interesting initial ideas. For example, how many of you are afraid that you are going to go down the bathtub drain? Hopefully, none of you do! But a 3-year-old might really worry about this as they sit at the front of the bathtub. A child might protest if told that something will happen “tomorrow” but be willing to accept an explanation that an event will occur “today after we sleep.” Or the young child may ask, “How long are we staying? From here to here?” while pointing to two points on a table. Concepts such as tomorrow, time, size, and distance are not easy to grasp at this young age. Understanding size, time, distance, fact, and fiction are all tasks that are part of cognitive development in the preschool years.
Preoperational Intelligence (Ob 5)

Piaget’s theory of cognitive development has a stage that coincides with early childhood known as the Preoperational Stage. According to Piaget, this stage occurs from the age of 2 to around 7 years. In the preoperational stage, children use symbols to represent words, images, and ideas, which is why children in this stage engage in pretend play. A child’s arms might become airplane wings as she zooms around the room, or a child with a stick might become a brave knight with a sword. Children also begin to use language in the preoperational stage, but they cannot understand adult logic or mentally manipulate information. The term operational refers to logical manipulation of information, so children at this stage are considered pre-operational. Children’s logic is based on their own personal knowledge of the world so far, rather than on conventional knowledge.
Let’s examine some Piaget’s assertions about children’s cognitive abilities during the Preoperational Stage.
Pretend Play: Pretending is a favorite activity at this time. A toy has qualities beyond the way it was designed to function and can now be used to stand for a character or object unlike anything originally intended. A teddy bear, for example, can be a baby or the queen of a faraway land!
Piaget believed that children’s pretend play helped children solidify new schemes they were developing cognitively. This play, then, reflected changes in their conceptions or thoughts. However, children also learn as they pretend and experiment. Their play does not simply represent what they have taught (Berk, 2007).
Egocentrism: Egocentrism in early childhood refers to the tendency of young children to think that everyone sees things in the same way as the child. For example, 10-year-old Keiko’s birthday is coming up, so her mom takes 3-year-old Kenny to the toy store to choose a present for his sister. He selects an Iron Man action figure for her, thinking that if he likes the toy, his sister will too. Piaget’s classic experiment on egocentrism involved showing children a 3-dimensional model of a mountain and asking them to describe what a doll that is looking at the mountain from a different angle might see. Children tend to choose a picture that represents their own, rather than the doll’s view. By age 7 children are less self-centered. Additionally, when children are speaking to others, they tend to use different sentence structures and vocabulary when addressing a younger child or an older adult. This indicates some awareness of the views of others.
Animism: Animism refers to attributing lifelike qualities to objects. An example could be a child believing that the sidewalk was mad and made them fall down, or that the stars twinkle in the sky because they are happy. To the imaginative child, the cup is alive, the chair that falls down and hits the child’s ankle is mean, and the toys need to stay home because they are tired. Cartoons frequently show objects that appear alive and take on lifelike qualities. Young children do seem to think that objects that move may be alive but after age 3, they seldom refer to objects as being alive (Berk, 2007).

Classification Errors: Preoperational children have difficulty understanding that an object can be classified in more than one way. Classification is the ability to simultaneously sort things into general and more specific groups, using different types of comparisons. For example, if shown three white buttons and four black buttons and asked whether there are more black buttons or white buttons or buttons, the child is likely to respond that there are more black buttons. The child does not identify the category of buttons being larger than each subgroup (black and white) indicating a lack of hierarchy classification. Most children develop hierarchical classification ability between the ages of 7 and 10. As the child’s vocabulary improves and more schemes are developed, the ability to classify objects improves.
Conservation Errors: Children in the preoperational stage do not understand conversation. Conservation refers to the ability to recognize that moving or rearranging matter does not change the quantity. Imagine a 2-year-old and 4-year-old eating lunch. The 4-year-old has a whole peanut butter and jelly sandwich. He notices, however, that his younger sister’s sandwich is cut in half and protests, “She has more!” This is a conservation error of number. He does not realize that 2 half sandwiches make a whole sandwich. Often children who fail conservation errors will concentrate on one aspect (focusing on number of sandwiches verses the total size (or mass)). Centration is the act of focusing all attention on one characteristic or dimension of a situation while disregarding all others. He is exhibiting centration by focusing on the number of pieces, which results in a conservation error.
The classic Piagetian experiment associated with conservation involves liquid (Crain, 2005). The child usually notes that the beakers do contain the same amount of liquid. When one of the beakers is poured into a taller and thinner container, children who are younger than seven or eight years old typically say that the two beakers no longer contain the same amount of liquid, and that the taller container holds the larger quantity (centration), without taking into consideration the fact that both beakers were previously noted to contain the same amount of liquid.
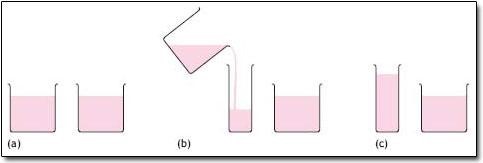
Irreversibility is also demonstrated during this stage and is closely related to the ideas of centration and conservation. Irreversibility refers to the young child’s difficulty mentally reversing a sequence of events. In the same beaker situation, the child does not realize that, if the sequence of events was reversed and the water from the tall beaker was poured back into its original beaker, then the same amount of water would exist.
| Conservation Errors Revisited.
Let’s look at Kenny and Keiko again. Dad gave a slice of pizza to 10-year-old Keiko and another slice to 3-year-old Kenny. Kenny’s pizza slice was cut into five pieces, so Kenny told his sister that he got more pizza than she did. Kenny did not understand that cutting the pizza into smaller pieces did not increase the overall amount. Kenny focused on the five pieces of pizza to his sister’s one piece even though the total amount was the same. What error was Kenny making? |
Centration, conservation errors, and irreversibility are indications that young children are reliant on visual representations. Because children have not developed this understanding of conservation, they cannot perform mental operations (a requirement for Piaget’s next stage).
Critique of Piaget: Similar to the critique of the sensorimotor period, several psychologists have attempted to show that Piaget also underestimated the intellectual capabilities of young children. For example, children’s specific experiences can influence when they are able to conserve. Children of pottery makers in Mexican villages know that reshaping clay does not change the amount of clay at much younger ages than children who do not have similar experiences (Price-Williams et al., 1969). Crain (2005) indicated that preoperational children could think rationally on mathematical and scientific tasks, and they are not as egocentric as Piaget implied. Research on Theory of Mind (discussed later in the chapter) has demonstrated that children overcome egocentrism by 4 or 5 years of age, which is sooner than Piaget indicated.
Children & Learning – The Mozart Effect: Is there a cognitive advantage for children to listen to classical music?
I’m sure everyone has heard at some point in their life that listening to classical music supposedly makes one smarter. There are many different meanings you could interpret from that statement. Does classical music have a permanent effect in raising one’s IQ just by listening? Does it only improve intelligence for a short time after listening? What areas of intelligence is the music supposed to improve? These are all questions you should be asking when you hear a statement such as “listening to classical music makes kids smarter”. This topic became the infamous anomaly it is today from a Russian study in 1993. In this study 36 college students were split into 3 separate groups where each group would sit in a room either listening to Mozart, concentration therapy sounds, or complete silence for 10 minutes. After the 10 minutes was up they all would take a short intelligence quiz with special reasoning tasks. What this study found is that the Mozart listening group scored slightly higher on the test than the other 2 groups.
According to further research, including a meta-analysis (Chabis, 1999), what was found out is the music does not in fact have any benefit in raising one’s intelligence. The classical music puts the listener’s brain in a state of higher awareness than normal so when given a reasoning intelligence task, the listener is more aware and should perform slightly better. Listening to classical music while performing a task such as reading can in fact impair one’s ability to comprehend all the information read because the music distracts the mind when you may not even realize it (Yen-Ning Su, 2017). Another study done showed that learning how to play music very well can improve a person’s spatial intelligence (Bower, 2004). Overall, the relationship music can have on one’s intelligence is clear that it does not in any way raise it, rather it evokes the mind to be on its feet ready for a task.
Vygotsky’s Sociocultural Theory of Cognitive Development (Ob 7)
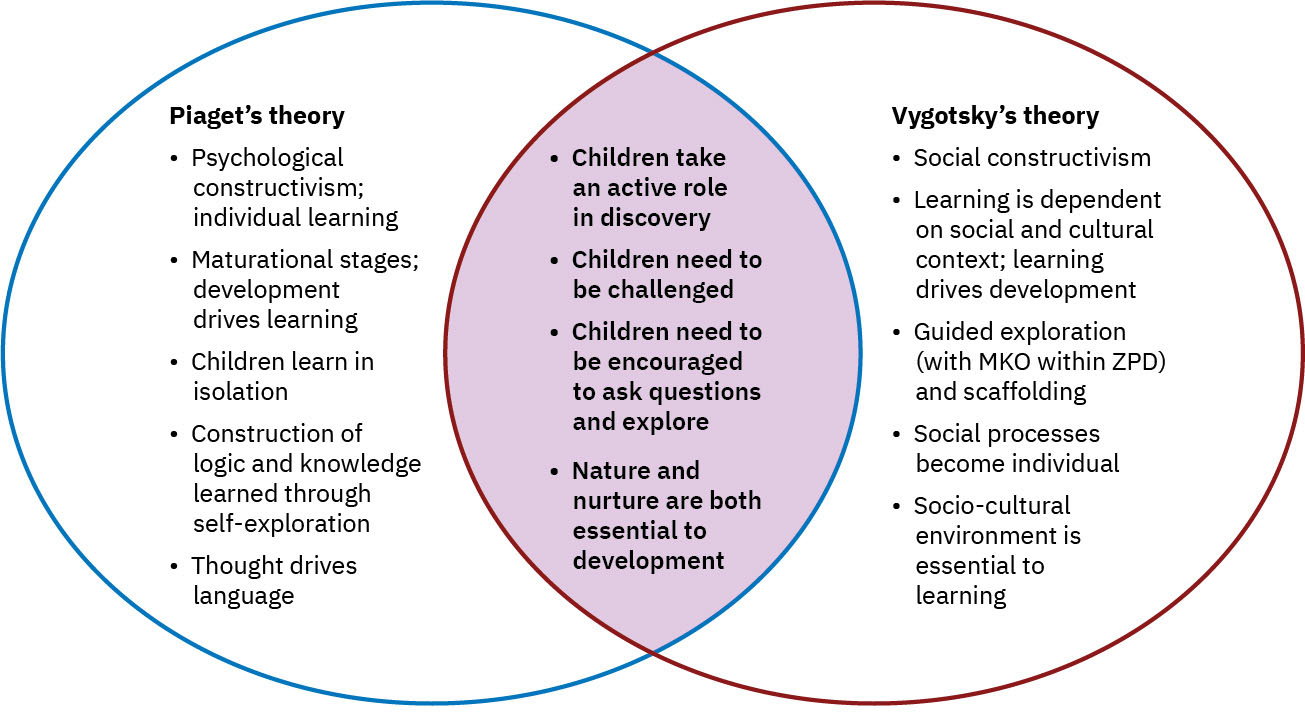
In contrast to Piaget on the child as the active learner, Lev Vygotsky argued that a child’s intrinsic development and the highest level of cognitive thinking is elicited from the language, writings, and concepts arising from the culture the child is surrounded by (Crain, 2005). He believed that social interactions with adults and more learned peers could facilitate a child’s potential for learning. Without this interpersonal instruction, he believed children’s minds would not advance very far as their knowledge would be based only on their own discoveries. Vygtosky’s theory including cultural and societal factors in learning go beyond supervision and peer relationships. They extend to the availability of resources such as books, tutors, mentors, and extra learning opportunities. Think about the ways that children learn to process information differently in varied sociocultural situations.
Below shows a comparison between Vygotsky’s theory and Piaget’s theory, although they identify learning takes different approaches, there are some shared concepts about learning.
Let’s review some of Vygotsky’s key concepts (as mentioned in chapter 2).
Zone of Proximal Development and Scaffolding: Vygotsky’s best-known concept is the Zone of Proximal Development (ZPD). Vygotsky stated that children should be taught in the ZPD, which occurs when they can almost perform a task, but not quite on their own without assistance. With the right kind of teaching, however, they can accomplish it successfully. A good teacher identifies a child’s ZPD and helps the child stretch beyond it. Then the adult (teacher) gradually withdraws support until the child can then perform the task unaided. Researchers have applied the metaphor of scaffolds (the temporary platforms on which construction workers stand) to this way of teaching. Scaffolding is the temporary support that parents or teachers give a child to do a task, sometimes the term guided participation is also used.

Private Speech: Do you ever talk to yourself? Why? Chances are, this occurs when you are struggling with a problem, trying to remember something or feel very emotional about a situation. Children talk to themselves too. Thinking out loud eventually becomes thought accompanied by internal speech (or private speech), and talking to oneself becomes a practice only engaged in when we are trying to learn something or remember something. This inner speech is not as elaborate as the speech we use when communicating with others (Vygotsky, 1962). Piaget interpreted this as Egocentric Speech or a practice engaged in because of a child’s inability to see things from another’s point of view. Vygotsky, however, believed that children talk to themselves in order to solve problems or clarify thoughts. As children learn to think in words, they do so aloud before eventually closing their lips and engaging in Private Speech or inner speech.
Theory of Mind (Ob 7)
Imagine showing a 3-year old child a Band-Aid box and asking the child what is in the box. Chances are, the child will reply, “Band-Aids.” Now imagine that you open the box and pour out crayons. If you ask the child what they thought was in the box before it was opened, they may respond, “crayons.” If you ask what a friend would have thought was in the box, the response would still be “crayons.” Why? Before about 4 years of age, a child does not recognize that the mind can hold ideas that are not accurate. So, this 3-year-old changes his or her response once shown that the box contains crayons. The theory of mind is the understanding that the mind can be tricked or that the mind is not always accurate. At around age 4, the child would reply, “Crayons” and understand that thoughts and realities do not always match.
Three-year-olds have difficulty distinguishing between what they once thought was true and what they now know to be true. They feel confident that what they know now is what they have always known (Birch & Bloom, 2003). For the theory of mind, a child must separate what he or she “knows” to be true from what someone else might “think” is true. In Piagetian terms, they must give up a tendency toward egocentrism. The child must also understand that what guides people’s actions and responses are what they “believe” rather than what is reality. In other words, people can mistakenly believe things that are false and will act based on this false knowledge. Consequently, prior to age 4 children are rarely successful at solving such a task (Wellman et al., 2001).

This awareness of the existence of mind is part of social intelligence or the ability to recognize that others can think differently about situations. It helps us to be self-conscious or aware that others can think of us in different ways and it helps us to be able to be understanding or empathetic toward others. This mind reading ability helps us to anticipate and predict the actions of others (even though these predictions are sometimes inaccurate). This is important for communication and social skills.
Autism Spectrum Disorder
The characteristics of Autism Spectrum Disorder (ASD) are seen during early childhood (as established by the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) (American Psychiatric Association, 2022). So, what exactly is Autism Spectrum Disorder?
Children with this disorder show signs of “persistent deficits in social communication and social interaction” and “restricted, repetitive patterns” of behavior (American Psychiatric Association, 2022). Children with ASD experience difficulties with explaining and predicting other people’s behavior, which leads to problems in social communication and interaction. Children who are diagnosed with an autistic spectrum disorder usually develop the theory of mind more slowly than other children and continue to have difficulties with it throughout their lives.
ASD occurs in around 17 percent of children and can manifest with a wide range of highly diverse symptoms and neurological characteristics (Centers for Disease Control and Prevention, 2024). The average age to receive a diagnosis is 4.5 years old, though many individuals are diagnosed at later ages, including in adulthood (Brett et al., 2016).
There are many possible signs of autism spectrum disorder, and the appearance of some does not imply ASD is present. However, early signs may warrant a referral to a specialist for professional assessment. The table shows possible signs for a four-year-old.
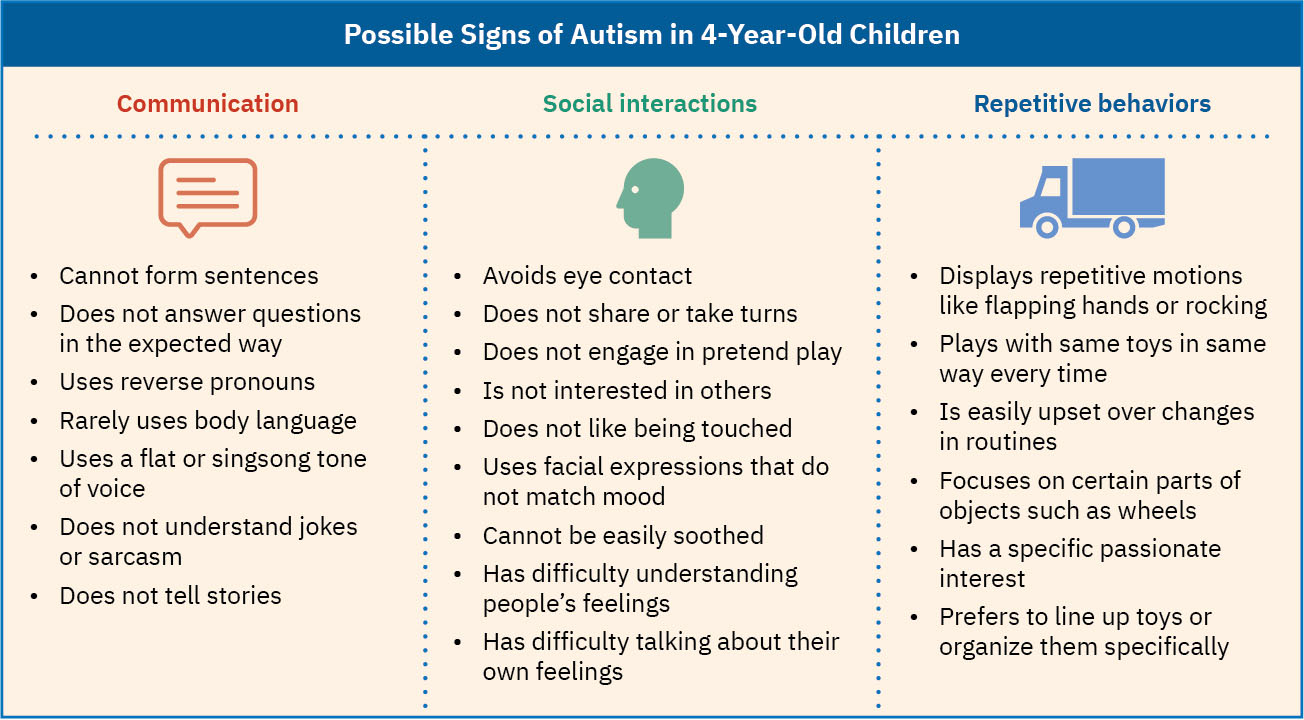
Some of the common traits that appear in early childhood are struggles with social interactions, particularly making eye contact, responding reciprocally, understanding the perspectives of others, and communicating verbally. These noticeable differences in social interactions among autistic preschoolers often result in parental concerns and referrals to specialists (see table above). Note that most psychologists use the phrase autistic preschooler (identity-first language) as opposed to person with autism spectrum disorder (person-first language) because a large percentage of allies and advocates in the autistic community have stated this language preference. The language and preferences for any neurodiversity or disorder vary by the individual and the represented community. When in doubt, always follow the lead of the person or ask their preference (Autistic Self Advocacy Network, n.d.; Ladau, 2021).

Beyond early childhood, those with autism spectrum disorders may follow unique developmental trajectories. TThe qualifier “spectrum” in autism spectrum disorder is used to indicate that individuals with the disorder can show a range, or spectrum, of symptoms that vary in their magnitude and severity: Some severe, others less severe. Though ASD is lifelong, some children develop skills like those of their non-autistic peers, whereas others may continue to struggle with particular social and emotional expectations across the lifespan (Elder et al., 2017). Some individuals with an autism spectrum disorder, particularly those with better language and intellectual skills, can live and work independently as adults.
Early diagnosis of Autism Spectrum Disorder
About half of parents of children with ASD notice their child’s unusual behaviors by age 18 months, and about four-fifths notice by age 24 months, but often a diagnosis comes later, and individual cases vary significantly. Typical early signs of autism include:
- No babbling by 12 months.
- No gesturing (pointing, waving, etc.) by 12 months.
- No single words by 16 months.
- No two-word (spontaneous, not just echolalic) phrases by 24 months.
- Loss of any language or social skills, at any age.
Information Processing in Early Childhood (Ob 6)
The information processing model examines how memory gets stored (mentioned in chapter 2). Information processing researchers focus on several issues in cognitive development for this age group, including improvements in attention skills, changes in the capacity and the emergence of executive functions in working memory. Additionally, in early childhood memory strategies, memory accuracy, and autobiographical memory emerge. Early childhood is seen by many researchers as a crucial time period in memory development (Posner & Rothbart, 2007).
Attention
Changes in attention have been described by many as the key to changes in human memory (Nelson & Fivush, 2004; Posner & Rothbart, 2007). However, attention is not a unified function; it is comprised of sub-processes. The ability to switch our focus between tasks or external stimuli is called divided attention or multitasking. This is separate from our ability to focus on a single task or stimulus while ignoring distracting information, called selective attention. Different from these is sustained attention, or the ability to stay on task for long periods of time. Moreover, we also have attention processes that influence our behavior and enable us to inhibit a habitual or dominant response and others that enable us to distract ourselves when upset or frustrated.
Divided Attention: Young children (age 3-4) have considerable difficulties in dividing their attention between two tasks, and often perform at levels equivalent to our closest relative, the chimpanzee, but by age 5 they have surpassed the chimp (Hermann et al., 2015; Hermann & Tomasello, 2015). Despite these improvements, 5-year-olds continue to perform below the level of school-age children, adolescents, and adults.
Selective Attention: Children’s ability with selective attention tasks improve as they age. However, this ability is also greatly influenced by the child’s temperament (Rothbart & Rueda, 2005), the complexity of the stimulus or task (Porporino et al., 2004), and along with whether the stimuli are visual or auditory (Guy et al., 2013). Guy et al. (2013) found that children’s ability to selectively attend to visual information outpaced that of auditory stimuli. This may explain why young children are not able to hear the voice of the teacher over the cacophony of sounds in the typical preschool classroom (Jones et al., 2015). Jones and his colleagues found that 4 to 7-year-olds could not filter out background noise, especially when its frequencies were close in sound to the target sound. In comparison, 8 to 11-year-old older children often performed similarly to adults.
Sustained Attention: Most measures of sustained attention typically ask children to spend several minutes focusing on one task, while waiting for an infrequent event, while there are multiple distractors for several minutes. Berwid et al. (2005) asked children between the ages of 3 and 7 to push a button whenever a “target” image was displayed, but they had to refrain from pushing the button when a non-target image was shown. The younger the child, the more difficulty he or she had maintaining their attention.
Memory
Based on studies of adults, people with amnesia, and neurological research on memory, researchers have proposed several “types” of memory.” Let’s examine changes in memory during early childhood.
Sensory memory (also called the sensory register): the first stage of the memory system, and it stores sensory input in its raw form for a very brief duration; essentially long enough for the brain to register and start processing the information. Studies of auditory sensory memory have found that the sensory memory trace for the characteristics of a tone lasts about one second in 2-year-olds, two seconds in 3-year-olds, more than two seconds in 4-year-olds and three to five seconds in 6-year-olds (Glass et al., 2008). Other researchers have found that young children hold sounds for a shorter duration than do older children and adults and that this deficit is not due to attentional differences between these age groups, but reflect differences in the performance of the sensory memory system (Gomes et al., 1999).
Short-term or working memory: The second stage of the memory system. Working memory is the component of memory in which current conscious mental activity occurs. Working memory often requires conscious effort and adequate use of attention to function effectively. As you read earlier, children in this age group struggle with many aspects of attention and this greatly diminishes their ability to consciously juggle several pieces of information in memory. The capacity of working memory, that is the amount of information someone can hold in consciousness, is smaller in young children than in older children and adults. The typical adult and teenager can hold a 7-digit number active in their short-term memory. The typical 5-year-old can hold only a 4-digit number active. This means that the more complex a mental task is, the less efficient a younger child will be in paying attention to, and actively processing, the information in order to complete the task.
Long-term memory also is known as permanent memory: the third component in memory. A basic division of long-term memory is between declarative and nondeclarative memory. Declarative memories, sometimes referred to as explicit memories, are memories for facts or events that we can consciously recollect. Nondeclarative memories sometimes referred to as implicit memories, are typically automated skills that do not require conscious recollection. Remembering that you have an exam next week would be an example of declarative memory. In contrast, knowing how to walk so you can get to the classroom or how to hold a pencil to write would be examples of non-declarative memories. Declarative memory is further divided into semantic and episodic memory. Semantic memories are memories for facts and knowledge that are not tied to a timeline, while episodic memories are tied to specific events in time.
A component of episodic memory is autobiographical memory or our personal narrative. Autobiographical memories are a subset of the declarative memory category. As you may recall from Chapter 4, the concept of infantile amnesia was introduced. Adults rarely remember events from the first few years of life. In other words, we lack autobiographical memories from our experiences as an infant, toddler, and very young preschooler. Several factors contribute to the emergence of autobiographical memory including brain maturation, improvements in language, opportunities to talk about experiences with parents and others, the development of the theory of mind, and a representation of “self” (Nelson & Fivush, 2004). 2-year-olds do remember fragments of personal experiences, but these are rarely coherent accounts of past events (Nelson & Ross, 1980). Between 2 and 2 ½ years of age, children can provide more information about past experiences. However, these recollections require considerable prodding by adults (Nelson & Fivush, 2004). Over the next few years, children will form more detailed autobiographical memories and engage in more reflection of the past.
Executive function (EF)
Self-regulatory processes, such as the ability to inhibit behavior or cognitive flexibility, that enable adaptive responses to new situations or to reach a specific goal, are aspects of executive function. Executive function skills gradually emerge during early childhood and continue to develop throughout childhood and adolescence. Like many cognitive changes, brain maturation, especially the prefrontal cortex, along with experience influence the development of executive function skills. A child, whose parents are warm and responsive, use scaffolding when the child is trying to solve a problem, and who provide cognitively stimulating environments for the child show higher executive function skills (Fay-Stammbach et al., 2014). For instance, scaffolding was positively correlated with greater cognitive flexibility at age 2 and inhibitory control at age 4 (Bibok et al., 2009).
Executive function also is related to the use and selection of mental strategies to aid their memory performance. For instance, simple rote rehearsal may be used to commit information to memory. Young children, however, often do not rehearse unless reminded to do so, and when they do rehearse, they often fail to use clustering rehearsal. In clustering rehearsal, the person rehearses previous material while adding in additional information. If a list of words is read out loud to you, you are likely to rehearse each word as you hear it along with any previous words you were given. Young children will repeat each word they hear, but often fail to repeat the prior words in the list. In Schneider et al. (2009) longitudinal study of 102 kindergarten children, the majority of children used no strategy to remember information, a finding that was consistent with previous research. As a result, their memory performance was poor when compared to their abilities as they aged and started to use more effective memory strategies.
Summary of three cognitive theories
We have discussed three theories that connect to changes in cognitive development. Below is a summary table reviewing each theories stance in how changes occur and how variation is considered.
Table Comparative Summary of Three Cognitive Theories
| Theme | Piaget | Information Processing | Vygotsky |
| Nature-Nurture | Maturation and experience = Nature and nurture |
Not emphasized | Environmental factors interact with biological structures= Nurture on nature |
| Continuous-Discontinuous | Discontinuous= Stages | Usually continuous | Continuous |
| Culture? | Not really | Not emphasized | Critical component |
| Individual diff.? | Universal stages | Not really but does explain variation | Yes |
Language Development (Ob 8)
Vocabulary growth: A child’s vocabulary expands between the ages of 2 to 6 from about 200 words to over 10,000 words through a process called fast-mapping. Words are easily learned by making connections between new words and concepts already known. The parts of speech that are learned depend on the language and what is emphasized. Children speaking verb-friendly languages such as Chinese and Japanese as well as those speaking English tend to learn nouns more readily. However, those learning less verb-friendly languages such as English seem to need assistance in grammar to master the use of verbs (Imai et al., 2008). Children are also very creative in creating their own words to use as labels such as a “nei-nei” for horse or “clopster” for lobster.
Literal meanings: Children can repeat words and phrases after having heard them only once or twice. But they do not always understand the meaning of the words or phrases. This is especially true of expressions or figures of speech which are taken literally. For example, two preschool-aged girls began to laugh loudly while listening to a tape-recording of Disney’s “Sleeping Beauty” when the narrator reports, “Prince Phillip lost his head!” They imagine his head popping off and rolling down the hill as he runs and searches for it. Or a classroom full of preschoolers hears the teacher say, “Wow! That was a piece of cake!” The children began asking “Cake? Where is my cake? I want cake!”
Overregularization: Children learn rules of grammar as they learn language but may apply these rules inappropriately at first. For instance, a child learns to add “ed” to the end of a word to indicate past tense. They form a sentence such as “I goed there. I doed that.” This is typical at ages 2 and 3. They will soon learn new words such as went and did to be used in those situations. It would seem that the child has solidly learned the grammar rule, but it is actually common for the developing child to revert back to their original mistake. This happens as they overregulate the rule. This can happen because they intuitively discover the rule and overgeneralize it or because they are explicitly taught to add “ed” to the end of a word to indicate past tense in school. A child who had previously produced correct sentences may start to form incorrect sentences such as, “I goed there. I doed that.” These children are able to quickly re-learn the correct exceptions to the -ed rule, and it is a sign of their language learning.
The Impact of Training: Remember Vygotsky and the Zone of Proximal Development? Children can be assisted in learning language by others who listen attentively, model more accurate pronunciations, and encourage elaboration. The child exclaims, “I’m goed there!” and the adult responds, “You went there? Say, ‘I went there.’ Where did you go?” Children may be ripe for language as Chomsky suggests, but active participation in helping them learn is important for language development as well. The process of scaffolding (Vygotsky’s theory) is one in which the guide provides needed assistance to the child as a new skill is learned.
Early Literacy
Phonological awareness, learning the sound system of a language, is the foundation for literacy, the ability to read, write, and understand information. Early literacy is enhanced by robust vocabulary development, phonological awareness, print awareness, and comprehension skills. Thus, children who have strong early literacy skills are more likely to enjoy academic success (Ramsook et al., 2020).
Parents and caregivers can support early literacy by reading to children regularly, supporting a text-rich environment with books and writing materials, and engaging in conversations and activities like storytelling and singing that promote language development. The repetition found in books and songs reinforces semantics, syntax, and grammar, and will promote a positive attitude towards reading. Reading books also furthers children’s exposure to a wider range of vocabulary than they might hear in everyday speech and conversations.
Although research has extensively explored older children’s use of tablets for reading, currently there is only limited understanding of the impact of digital reading in the early stages of literacy development. One review compared the impact of interactive, enhanced e-books (that is, with embedded dictionaries) to that of print books and non-enhanced, non-interactive e-books on the literacy skills of young children (López-Escriban et al., 2021). Most of the books in the study were carefully chosen by teachers for artistic and literary quality. The analysis revealed that when high-quality material is used, both enhanced and non-enhanced e-books are either equal to or have an advantage over print books in promoting phonological awareness and vocabulary learning. These findings have positive implications for marginalized populations, including those at risk of learning disabilities and those from lower SES families, and offer another alternative to standardized school-based instruction.
Psychosocial Development in Early Childhood: A Look at Self-Concept, Gender Identity, and Family Life
Self-Concept (Ob 11)
Early childhood is a time of forming an initial sense of self. Self-concept is our self-description according to various categories, such as our external and internal qualities. In contrast, self-esteem is an evaluative judgment about who we are. The emergence of cognitive skills in this age group results in improved perceptions of the self. If asked to describe yourself to others you would likely provide some physical descriptors, group affiliation, personality traits, behavioral quirks, and important values and beliefs. When researchers ask young children the same open-ended question, the children provide physical descriptors, preferred activities, and favorite possessions. Typically, a self-concept for a three-year-old will include basic vital facts such as their name, gender, and age. Thus, a 3-year-old might describe herself as a 3-year-old girl with red hair, who likes to play with Legos. This focus on external qualities is referred to as the categorical self. However, even children as young as 3 know there is more to themselves than these external characteristics. arter and Pike (1984) challenged the method of measuring personality with an open-ended question as they felt that language limitations were hindering the ability of young children to express their self-knowledge. They suggested a change to the method of measuring self-concept in young children, whereby researchers provide statements that ask whether something is true of the child (e.g., “I like to boss people around,” “I am grumpy most of the time”). Consistent with Harter and Pike’s suspicions, those in early childhood answer these statements in an internally consistent manner, especially after the age of 4 (Goodvin et al., 2008) and often give similar responses to what others (parents and teachers) say about the child (Brown et al., 2008; Colwell & Lindsey, 2003). Around age four, children may start to include new information in their self-concept, such as their interests and hobbies. One child may say they like Batman and coloring books, whereas another may mention dancing and the color yellow. However, at age four, these components are based on concrete, factual statements and are not evaluative. Starting around age five or six, some children might start to evaluate their skills internally, but expressing this view outwardly as part of their self-concept is still rare and will usually start later in childhood (Putnick et al., 2020).
Young children tend to have a generally positive self-image. When asked whether they perform better than, worse than, or about the same as other children when it comes to running, coloring, singing, or dancing, most four-year-olds rate themselves as performing better than others (Marsh et al., 2002; Orth et al., 2018). The reason is that at four years of age, most children are not yet able to fully consider the performance of others to make objective comparisons. Instead, they are most familiar with their own perspective and performance, and being satisfied with their abilities, they rate their own skills highly.
Herbert Mead (1967) explains how we develop a social sense of self by being able to see ourselves through the eyes of others. There are two parts of the self: the “I self” which is the part of the self that is spontaneous, creative, innate, and is not concerned with how others view us and the “me self” or the social definition of who we are. When we are born, we are all “I” and act without concern about how others view us. But the socialized self begins when we are able to consider how one important person views us. This initial stage is called “taking the role of the significant other.” For example, a child may pull a cat’s tail and be told by his mother, “No! Don’t do that, that’s bad” while receiving a slight slap on the hand. Later, the child may mimic the same behavior toward the self and say aloud, “No, that’s bad” while patting his own hand. What has happened? The child is able to see himself through the eyes of the mother. As the child grows and is exposed to many situations and rules of culture, he begins to view the self in the eyes of many others through these cultural norms or rules. This is referred to as “taking the role of the generalized other” and results in a sense of self with many dimensions. The child comes to have a sense of self as a student, as a friend, as a son, and so on.
Around five years of age, children start to become more self-conscious and are better able to evaluate and assess the way they are perceived by others. In many countries, including the United States, this coincides with the beginning of formal education. In a school setting, children may start to notice that some children are better at different activities, and perhaps they themselves are not the fastest or the best at everything. In the first year of formal education, children tend to experience an adjustment to their self-esteem, leading them to place less reliance on praise from parents and more on the social comparisons they make with other children (Pinto et al., 2015). It is typical to see self-esteem decline a little in the first year of formal education as children begin to have more realistic perceptions of themselves. For example, they may transform from believing they are “the highest jumper ever” to observing that they jump about as high as their peers in physical education class.
Self-Control
Self-control is not a single phenomenon but is multi-faceted. It includes response initiation, the ability to not initiate a behavior before you have evaluated all of the information, response inhibition, the ability to stop a behavior that has already begun, and delayed gratification, the ability to hold out for a larger reward by forgoing a smaller immediate reward (Dougherty et al., 2005). It is in early childhood that we see the start of self-control, a process that takes many years to fully develop. In the now classic “Marshmallow Test” (Mischel et al., 1972) children are confronted with the choice of a small immediate reward (immediate gratification) (a marshmallow) and a larger delayed reward (more marshmallows). Walter Mischel and his colleagues over the years have found that the ability to delay gratification at the age of 4 predicted better academic performance and health later in life (Mischel et al., 2011). The Marshmallow Test connects to children’s development of self-control and motivation. Self-control is related to executive function (term discussed earlier in the chapter). As executive function improves, children become less impulsive (Traverso et al., 2015) and self-regulate emotions, attention, and behavior.

Erikson: Initiative vs. Guilt (Ob 9)
By age three, the child begins stage 3: initiative versus guilt. The trust and autonomy of previous stages develop into a desire to take initiative or to think of ideas and initiate action. Children are curious at this age and start to ask questions so that they can learn about the world. Parents should try to answer those questions without making the child feel like a burden or implying that the child’s question is not worth asking. Children may want to build a fort with the cushions from the living room couch or open a lemonade stand in the driveway or make a zoo with their stuffed animals and issue tickets to those who want to come. Or they may just want to get themselves ready for bed without any assistance. To reinforce taking initiative, caregivers should offer praise for the child’s efforts and avoid being critical of messes or mistakes. Soggy washrags and toothpaste left in the sink pales in comparison to the smiling face of a 5-year-old that emerges from the bathroom with clean teeth and pajamas!
During this time, children are taking initiative but also may desire having set routines. Many young children desire consistency and may be upset if there are changes to their daily routines. They may like to line up their toys or other objects or place them in symmetric patterns. Many young children have a set bedtime ritual and a strong preference for certain clothes, toys or games. All these tendencies tend to wane as children approach middle childhood, and the familiarity of such ritualistic behaviors seem to bring a sense of security and a general reduction in childhood fears and anxiety (Evans et al., 1999; Evans & Leckman, 2015).
It is possible that the child will not be happy with helping to clean, and the child may even become aggressive or angry, but it is important to remember that the child is still learning how to navigate their world. They are trying to build a sense of autonomy, and they may not react well when they are asked to do something that they had not planned. Parents should be aware of this, and try to be understanding, but also be firm. Guilt for a situation where a child did not do their best allows a child to understand their responsibilities, see their potential, and helps the child learn to exercise self-control. The goal is to find a balance between initiative and guilt, not a free-for-all where the parent allows the child to do anything they want to. The parent must guide the child if they are to have a successful resolution in this stage. A parenting practice is to emphasize a when bad choice and redirect verses shutting down their desire to initiate or feeling he/she is bad.
Gender Identity, Gender Constancy, and Gender Roles (Ob 12)
Gender refers to the attitudes, feelings, and behaviors that a given culture associates with a person’s biological sex (APA, 2012). Another important dimension of the self is the sense of self as male or female. Gender identity is a person’s deeply‐felt, inherent sense of being a boy, a man, or male; a girl, a woman, or female; or an alternative gender (e.g., genderqueer, gender nonconforming, gender neutral) that may or may not correspond to a person’s sex assigned at birth or to a person’s primary or secondary sex characteristics. Since gender identity is internal, a person’s gender identity is not necessarily visible to others.
Gender identity takes on more meaning during the preschool years as children are becoming increasingly interested in finding out the differences between boys and girls both physically and in terms of what activities are acceptable for each. While 2-year-olds can identify some differences and learn whether they are boys or girls, preschoolers become more interested in what it means to be male or female. Children begin to connect the concept “girl” or “boy” to specific attributes. They form stronger rules or expectations for how each gender behaves and looks (Kuhn et al., 1978; Martin et al., 2004; Halim & Ruble, 2010). By age three, most can label their gender, in most cases as girl or boy (Bem, 1981; Bem, 1983). At approximately age 4, children acquire gender stability, which is the understanding that, for most people, boys grow up to be men, that girls grow up to be women, and that gender is a stable concept. However, at this age it is also common for children to assume that temporary changes in appearance, actions, or social roles can alter someone’s gender and change gender stability. For instance, they may think a girl who cuts her hair short is now a boy, or that a boy who practices ballet has become a girl.
This self-identification or gender identity is followed sometime later with gender constancy or the knowledge that gender does not change. By age six, children understand gender constancy, which is the belief that gender is resilient across contexts and situations, and immune to superficial changes like altered hairstyles or clothing and violations of gender expectations. Though these three realizations about gender are normative markers of gender development, individual differences and the diverse environments children experience will somewhat influence the age at which they are reached (Martin & Ruble, 2010). However, around ages 5-6 years-old, children’s thinking may be rigid in many ways for defining gender. For example, 5- and 6-year-olds are very aware of rules and of the pressure to comply with them. They do so rigidly because they are not yet developmentally ready to think more deeply about the beliefs and values that many rules are based on. For example, as early educators and parents know, the use of “white lies” is still hard for them to understand. Researchers call these ages the most “rigid” period of gender identity (Weinraub et al., 1984; Egan et al., 2001; Miller et al., 2009). A child who wants to do or wear things that are not typical of his gender is probably aware that other children find it strange. The persistence of these choices, despite the negative reactions of others, show that these are strong feelings. Gender rigidity typically declines as children age (Trautner et al., 2005; Halim et al., 2013). With this change, children develop stronger moral impulses about what is “fair” for themselves and other children (Killen & Stangor, 2001). As neurological and cognitive development continue and as children gain more social experiences in the world, they begin to understand nuances in rules and become less judgmental and enforcing of gender norms.
Part of gender identity is the formation of gender roles. Gender roles, or the rights and expectations that are associated with being male or female, are learned throughout childhood and into adulthood. Behavior that is compatible with cultural expectations is referred to as gender‐normative; behaviors that are viewed as incompatible with these expectations constitute gender nonconformity (APA, 2012). One of the greatest influences in early childhood in understanding gender roles comes from family members and caregivers as children infer differences between them as being due to gender. That is, if dad washes the dishes and mom mows the lawn, they assume dishes are boys’ work and lawn care is for girls, even if the division of labor is a factor of skills, preferences, or schedules. These patterns and observations are highly similar across children in gay, lesbian, and heterosexual families (Bos & Sandfort, 2010; Goldberg et al., 2012). Media is also a source of information. Although parents and caregivers often curate some of the media to which children are exposed—such as by selecting films, video games, and technology—children are constantly bombarded with color-coded advertisements and shopping aisles filled with gender-specific products, and subtle nods to gender norms that parents may miss.

Children begin to understand and internalize gender roles and stereotypes from a wide range of sources including their families, the media, and peers. Watch this video in which children explain some of the ways they’ve come to understand gender to learn more.
Learning through reinforcement and modeling: Learning theorists (chapter 2) suggest that gender role socialization is a result of the ways in which parents, teachers, friends, schools, religious institutions, media, and others send messages about what is acceptable or desirable behavior as males or females. This socialization begins early-in fact, it may even begin the moment a parent learns that a child is on the way. Knowing the sex of the child can conjure up images of the child’s behavior, appearance, and potential on the part of a parent. And this stereotyping continues to guide perception through life. Consider parents of newborns, shown a 7-pound, 20-inch baby, wrapped in blue (a color designating males) describe the child as tough, strong, and angry when crying. Shown the same infant in pink (a color used in the United States for baby girls), these parents are likely to describe the baby as pretty, delicate, and frustrated when crying (Maccoby & Jacklin, 1987). Female infants are held more, talked to more frequently, and given direct eye contact, while male infants play is often mediated through a toy or activity.
Sons are given tasks that take them outside the house and that have to be performed only on occasion while girls are more likely to be given chores inside the home such as cleaning or cooking that is performed daily. Sons are encouraged to think for themselves when they encounter problems and daughters are more likely to be given assistance even when they are working on an answer. This impatience is reflected in teachers waiting less time when asking a female student for an answer than when asking for a reply from a male student (Sadker & Sadker, 1994). Girls are given the message from teachers that they must try harder and endure in order to succeed while boys’ successes are attributed to their intelligence. Friends discuss what is acceptable for boys and girls and popularity may be based on modeling what is considered ideal behavior or looks for the sexes. Girls tend to tell one another secrets to validate others as best friends while boys compete for position by emphasizing their knowledge, strength, or accomplishments. This focus on accomplishments can even give rise to exaggerating accomplishments in boys, but girls are discouraged from showing off and may learn to minimize their accomplishments as a result. Of course, the stereotypes can influence which kinds of courses or vocational choices girls and boys are encouraged to make. We are recipients of these cultural expectations, but may also modify these roles (Kimmel, 2008).

How much does gender matter? In the United States, gender differences are found in school experiences (even into college and professional school, girls are less vocal in the classrooms and much more at risk for sexual harassment from teachers, coaches, classmates, and professors), in social interactions and in media messages. The stereotypes that boys should be strong, forceful, active, dominant, and rational and that girls should be pretty, subordinate, unintelligent, emotional, and talkative are portrayed in children’s toys, books, commercials, video games, movies, television shows, and music. In adulthood, these differences are reflected in income gaps between men and women where women working full-time earn about 74 percent the income of men, in higher rates of women suffering rape and domestic violence, higher rates of eating disorders for females, and in higher rates of violent death for men in young adulthood. Each of these differences will be explored further in subsequent chapters.
The impact in other parts of the world: Gender differences in India and China can be a matter of life and death as preferences for male children have been strong historically and are still held, especially in rural areas (WHO, 2010). Male children are given preference for receiving food, breast milk, medical care, and other resources. It is no longer legal to give parents information on the sex of their developing child for fear that they will abort a female fetus. Clearly, gender socialization and discrimination still impact development in a variety of ways across the globe.
Gender Dysphoria: A growing body of research is now focused on gender dysphoria, or the distress accompanying a mismatch between one’s gender identity and biological sex (APA, 2013). Gender Dysphoria as a diagnosis characterized by “a marked incongruence between” a person’s gender assigned at birth and gender identity (American Psychiatric Association, 2013, p. 453). Gender Dysphoria replaced the diagnosis of Gender Identity Disorder (GID) in the previous version of the DSM (APA, 2000). Although prevalence rates are low, at approximately 0.3 percent of the United States population (Russo, 2016), children who later identified as transgender, often stated that they were the opposite gender as soon as they began talking. Comments such as stating they prefer the toys, clothing, and anatomy of the opposite sex while rejecting the toys, clothing, and anatomy of their assigned sex are criteria for a diagnosis of Gender Dysphoria in children. Certainly, many young children do not conform to the gender roles modeled by the culture and even push back against assigned roles. However, they do not experience discomfort regarding their gender identity and would not be identified with Gender Dysphoria. A more comprehensive description of Gender Dysphoria, including current treatments, will be discussed in the chapter on adolescence.
Diagnostic criteria for gender dysphoria in children include significant distress or impairment due to marked gender incongruence, such as a strong desire to be-or a belief that one is the other gender; preference for the toys, games, roles, and activities stereotypically associated with the other gender, and a strong dislike of one’s sexual anatomy (APA, 2013).
Family Life
Parenting Styles (Ob 9)
Relationships between parents and children continue to play a significant role in children’s development during early childhood. We will explore two models of parenting styles. Keep in mind that these most parents do not follow any model completely. Real people tend to fall somewhere in between these styles. And sometimes parenting styles change from one child to the next or in times when the parent has more or less time and energy for parenting. Parenting styles can also be affected by concerns the parent has in other areas of his or her life. For example, parenting styles tend to become more authoritarian when parents are tired and perhaps more authoritative when they are more energetic. Sometimes parents seem to change their parenting approach when others are around, maybe because they become more self-conscious as parents or are concerned with giving others the impression that they are a “tough” parent or an “easy-going” parent. And of course, parenting styles may reflect the type of parenting someone saw modeled while growing up.
Baumrind (1971) offers a model of parenting that is four styles and measured along levels of responsiveness and demand. In general, children develop greater competence and self-confidence when parents have high, but reasonable expectations for children’s behavior, communicate well with them, are warm, loving, and responsive, and use reasoning, rather than coercion as preferred responses to children’s misbehavior. This kind of parenting style has been described as Authoritative (Baumrind, 2013). Authoritative parents are supportive and show interest in their kids’ activities, but are not overbearing and allow them to make constructive mistakes. Parents allow negotiation where appropriate, and consequently, this type of parenting is considered more democratic. Authoritarian, is the traditional model of parenting in which parents make the rules and children are expected to be obedient. Baumrind suggests that authoritarian parents tend to place maturity demands on their children that are unreasonably high and tend to be aloof and distant. Consequently, children reared in this way may fear rather than respect their parents and, because their parents do not allow discussion, may take out their frustrations on safer targets-perhaps as bullies toward peers. Permissive parenting involves holding expectations of children that are below what could be reasonably expected from them. Children are allowed to make their own rules and determine their own activities. Parents are warm and communicative, but provide little structure for their children. Children fail to learn self-discipline and may feel somewhat insecure because they do not know the limits. Uninvolved parents are disengaged from their children. They do not make demands on their children and are non-responsive. These children can suffer in school and in their relationships with their peers (Gecas & Self, 1991).
Table. Baumrind’s Parenting Style Dimensions classified by Warmth & Control
| Demand/Control | |||
| Warmth/Responsiveness | Low | High | |
| Low | Uninvolved | Authoritarian | |
| High | Permissive | Authoritative | |
Table. Summary of Baumrind’s Parenting Styles
| Parenting Style | Characteristics |
| Authoritative Style | The parent gives reasonable demands and consistent limits express warmth and affection and listens to the child’s point of view.
Parents set rules and explain the reasons behind them, but are also flexible and willing to make exceptions to the rules in certain cases. This is the style most encouraged in modern American society. American children raised by authoritative parents tend to have high self-esteem and social skills. Effective parenting styles vary as a function of culture and, as Small (1999) points out, the authoritative style is not necessarily preferred or appropriate in all cultures. |
| Authoritarian Style | The parent places a high value on conformity and obedience. The parents are often strict, tightly monitor their children, and express little warmth.
Authoritarian parents probably would not make exceptions to rules because they consider the rules to be set, and they expect obedience. This style can create anxious, withdrawn, and unhappy kids. Authoritarian parenting is as beneficial as the authoritative style in some ethnic groups. For instance, first-generation Chinese American children raised by authoritarian parents did just as well in school as their peers who were raised by authoritative parents. |
| Permissive Style | Permissive parents make few demands and rarely use punishment; the kids run the show and anything goes. There are rarely strict rules set for behavior.
The parents tend to be very nurturing and loving and may play the role of a friend rather than the parent. Children raised by permissive parents tend to lack self- discipline, and the permissive parenting style is negatively associated with grades. The permissive style may also contribute to other risky behaviors such as alcohol abuse, risky sexual behavior especially among female children, and increased the display of disruptive behaviors by male children. There are some positive outcomes associated with children raised by permissive parents, such as higher self-esteem, better social skills, and lower levels of depression. |
| Uninvolved Style | The parents are indifferent, uninvolved, and sometimes referred to as neglectful. These parents may provide for the child’s basic needs, but little else.
The parents don’t respond to the child’s needs and make relatively few demands. This could be because of severe depression or substance abuse, or other factors such as the parents’ extreme focus on work. The children raised in this parenting style are usually emotionally withdrawn, fearful, anxious, perform poorly in school, and are at an increased risk of substance abuse. |

These four categories are along a continuum and real people tend to fall somewhere in between these styles. Sometimes parenting styles change from one child to the next or in times when the parent has more or less time and energy for parenting. Parenting styles can also be affected by concerns the parent has in other areas of his or her life. For example, parenting styles tend to become more authoritarian when parents are tired and perhaps more authoritative when they are more energetic. Sometimes parents seem to change their parenting approach when others are around, maybe because they become more self-conscious as parents or are concerned with giving others the impression that they are a “tough” parent or an “easy-going” parent. Additionally, parenting styles may reflect the type of parenting someone saw modeled while growing up.
Lemasters and Defrain (1989) offer another model of parenting. This model is interesting because it looks more closely at the motivations of the parent and suggests that parenting styles are often designed to meet the psychological needs of the parent rather than the developmental needs of the child.
- The martyr is a parent who will do anything for the child; even tasks that the child should do for himself or herself. All of the good deeds performed for the child, in the name of being a “good parent,” may be used later should the parent want to gain compliance from the child. If a child goes against the parent’s wishes, the parent can remind the child of all of the times the parent helped the child and evoke a feeling of guilt so that the child will do what the parent wants. The child learns to be dependent and manipulative as a result. (Beware! A parent busy whipping up cookies may really be thinking “control!”)
- The pal is like the permissive parent described in Baumrind’s model above. The pal wants to be the child’s friend. Perhaps the parent is lonely or perhaps the parent is trying to win a popularity contest against an ex-spouse. Pals let children do what they want and focus most on being entertaining and fun and set few limitations. Consequently, the child may have little self-discipline and may try to test limits with others.
- The police officer/drill sergeant style of parenting is similar to the authoritarian parent described above. The parent focuses primarily on making sure that the child is obedient and that the parent has full control of the child. Sometimes this can be taken to the extreme by giving the child tasks that are really designed to check on their level of obedience. For example, the parent may require that the child fold the clothes and place items back in the drawer in a particular way. If not, the child might be scolded or punished for not doing things “right.” This type of parent has a very difficult time allowing the child to grow and learn to make decisions independently. And the child may have a lot of resentment toward the parent that is displaced on others.
- The teacher-counselor parent is one who pays a lot of attention to expert advice on parenting and who believes that as long as all of the steps are followed, the parent can rear a perfect child. “What’s wrong with that?” you might ask. There are two major problems with this approach. First, the parent is taking all of the responsibility for the child’s behavior-at least indirectly. If the child has difficulty, the parent feels responsible and thinks that the solution lies in reading more advice and trying more diligently to follow that advice. Parents can certainly influence children, but thinking that the parent is fully responsible for the child’s outcome if faulty. A parent can only do so much and can never have full control over the child. Another problem with this approach is that the child may get an unrealistic sense of the world and what can be expected from others. For example, if a teacher-counselor parent decides to help the child build self-esteem and has read that telling the child how special he or she is or how important it is to compliment the child on a job well done, the parent may convey the message that everything the child does is exceptional or extraordinary. A child may come to expect that all of his efforts warrant praise and in the real world, this is not something one can expect. Perhaps children get more of a sense of pride from assessing their own performance than from having others praise their efforts.

- Lemasters and Defrain (1989) suggest that the athletic coach style of parenting is best. Before you draw conclusions here, set aside any negative experiences you may have had with coaches in the past. The principles of coaching are what are important to Lemasters and Defrain. A coach helps players form strategies, supports their efforts, gives feedback on what went right and what went wrong, and stands at the sideline while the players perform. Coaches and referees make sure that the rules of the game are followed and that all players adhere to those rules. Similarly, the athletic coach as a parent helps the child understand what needs to happen in certain situations whether in friendships, school, or home life and encourages and advises the child about how to manage these situations. The parent does not intervene or do things for the child. Rather, the parent’s role is to provide guidance while the child learns first-hand how to handle these situations. And the rules for behavior are consistent and objective and presented in that way. So, a child who is late for dinner might hear the parent respond in this way, “Dinner was at six o’clock.” Rather than, “You know good and well that we always eat at six. If you expect me to get up and make something for you now, you have got another thing coming! Just who do you think you are showing up late and looking for food? You’re grounded until further notice!” The most important thing to remember about parenting is that you can be a better, more objective parent when you are directing your actions toward the child’s needs and while considering what they can reasonably be expected to do at their stage of development. Parenting is more difficult when you are tired and have psychological needs that interfere with the relationship. Some of the best advice for parents is to try not to take the child’s actions personally and be as objective as possible.
Culture and Child-Rearing
The impact of culture cannot be ignored when examining parenting styles. A large study (Deater-Deckard et al., 2011) investigated the role of individualism and collectivism on parenting styles in nine countries and found that these cultural values played a large role on the extent to which parents prioritized control and/or warmth in caregiving for their children.
Responsiveness and demandingness are culturally based where warmth is responsive praise in America and control take the form of explaining and some form of choice. The two models of parenting described above assume that authoritative and athletic coaching styles are best because they are designed to help the parent raise a child who is independent, self-reliant, and responsible (connected to our cultural value of independence). However, outside of Western cultures, authoritative parenting style is rare. These are qualities favored in “individualistic” cultures such as the United States, particularly by the middle class. African-American, Hispanic, and Asian parents tend to be more authoritarian than non-Hispanic whites. Asian cultures have a tradition of filial piety where children are to respect, obey, and revere authority in greater regard than in the West. Baumrind’s theory of parenting styles often suggests that authoritative or democratic parenting is the most advantageous. However, in studies of children growing up in urban, high-crime areas, some researchers found that strict and authoritarian parenting may be an adaptive approach to reducing some risky behaviors (Clark et al., 2015). However, more recent research has suggested that strict and harsh parenting is not necessarily the optimal strategy, and that high levels of warmth and parent childrearing knowledge may be more effective prevention and intervention strategies for youth across classes, races, and ethnicities (Climent-Galarza et al., 2022; Mowen & Schroeder, 2018; Pinquart & Kauser, 2018; Roubinov & Boyce, 2017; Villarejo et al., 2024).
In Latino cultural beliefs, familismo emphasizes love, closeness, and mutual obligations of Latino family life. Authoritarian parenting has been used historically and reflects a cultural need for children to do as they are told. In societies where family members’ cooperation is necessary for survival, as in the case of raising crops, rearing children who are independent and who strive to be on their own makes no sense. But in an economy based on being mobile in order to find jobs and where one’s earnings are based on education, raising a child to be independent is very important.
Support for autonomy may be advantageous for parents who are raising children in individualistic cultures in which self-responsibility and independence are valued. However, In “collectivistic” cultures such as China or Korea, being obedient and compliant are favored behaviors. For parents in China and Korea, the use of control and boundaries tends to be a better predictor of positive child outcomes such as social emotional competence and academic achievement (Yim, 2022). This may be due to cultural emphasis on collectivism, or the upholding of group well-being over individual well-being.
Even within the U.S., socioeconomic status can also impact parenting practices. Working class parents are more likely than middle-class parents to focus on obedience and honesty when raising their children. In a classic study on social class and parenting styles called Class and Conformity, Kohn (1977) explains that parents tend to emphasize qualities that are needed for their own survival when parenting their children. Working class parents are rewarded for being obedient, reliable, and honest in their jobs. They are not paid to be independent or to question the management; rather, they move up and are considered good employees if they show up on time, do their work as they are told, and can be counted on by their employers. Consequently, these parents reward honesty and obedience in their children. Middle-class parents who work as professionals are rewarded for taking initiative, being self-directed, and assertive in their jobs. They are required to get the job done without being told exactly what to do. They are asked to be innovative and to work independently. These parents encourage their children to have those qualities as well by rewarding independence and self-reliance. Parenting styles can reflect many elements of culture.
Sibling Relationships
Siblings spend a considerable amount of time with each other and offer a unique relationship that is not found with same-age peers or with adults. Siblings play an important role in the development of social skills. Cooperative and pretend play interactions between younger and older siblings can teach empathy, sharing, and cooperation (Pike et al., 2005), as well as, negotiation and conflict resolution (Abuhatoum & Howe, 2013). However, the quality of sibling relationships is often mediated by the quality of the relationship and the psychological adjustment of the child (Pike et al., 2005). For instance, more negative interactions between siblings have been reported in families where parents had poor patterns of communication with their children (Brody et al., 1994). Children who have emotional and behavioral problems are also more likely to have negative interactions with their siblings. However, the psychological adjustment of the child can sometimes reflect the parent-child relationship. Thus, when examining the quality of sibling interactions, it is often difficult to tease out the separate effect of adjustment from the effect of the parent-child relationship.

Learn more: Our siblings are our first playmates. Watch this YouTube video about the impact of siblings on child development to learn more (Sea Lab Psychology, 2022).
While parents want positive interactions between their children, conflicts are going to arise, and some confrontations can be the impetus for growth in children’s social and cognitive skills. The sources of conflict between siblings often depend on their respective ages. Dunn and Munn (1987) revealed that over half of all sibling conflicts in early childhood were disputes about property rights. By middle childhood this starts shifting toward control over social situations, such as what games to play, disagreements about facts or opinions, or rude behavior (Howe et al., 2002). Researchers have also found that the strategies children use to deal with conflict change with age, but that this is also tempered by the nature of the conflict. Abuhatoum and Howe (2013) found that coercive strategies (e.g., threats) were preferred when the dispute centered on property rights, while reasoning was more likely to be used by older siblings and in disputes regarding control over the social situation. However, younger siblings also use reasoning, frequently bringing up the concern of legitimacy (e.g., “You’re not the boss”) when in conflict with an older sibling. This is a very common strategy used by younger siblings and is possibly an adaptive strategy in order for younger siblings to assert their autonomy (Abuhatoum & Howe, 2013). A number of researchers have found that children who can use non-coercive strategies are more likely to have a successful resolution, whereby a compromise is reached and neither child feels slighted (Ram & Ross, 2008; Abuhatoum & Howe, 2013). Not surprisingly, friendly relationships with siblings often lead to more positive interactions with peers. The reverse is also true. A child can also learn to get along with a sibling, with, as the song says “a little help from my friends” (Kramer & Gottman, 1992).
Birth Order is an Important Factor that Impacts Children’s Personality and Identity
|
Play
Freud, Vygotsky, and Piaget all saw play as providing positive outcomes for children. Parten (1932) observed 2 to 5-year-old children and noted six types of play. Three types she labeled as non-social (unoccupied, solitary, and onlooker) and three types were categorized as social play (parallel, associative, and cooperative). Younger children engage in non-social play more than those older; by age five associative and cooperative play are the most common forms of play (Dyer & Moneta, 2006).

Table. Parten’s Classification of Types of Play in Preschool Children
| Unoccupied Play | Children’s behavior seems more random and without a specific goal. This is the least common form of play. |
| Solitary Play | Children play by themselves, do not interact with others, nor are they engaging in similar activities as the children around them. |
| Onlooker Play | Children are observing other children playing. They may comment on the activities and even make suggestions, but will not directly join the play. |
| Parallel Play | Children play alongside each other, using similar toys, but do not directly act with each other. |
| Associative Play | Children will interact with each other and share toys, but are not working toward a common goal. |
| Cooperative Play | Children are interacting to achieve a common goal. Children may take on different tasks to reach that goal. |
Cross-cultural Differences in Play
Early childhood play activities vary widely across cultures, influenced by factors such as social norms, beliefs, values, and geographical location (Sims & Hutchins, 2011). For example, some cultures may place a greater emphasis on physical play such as running, jumping, and climbing, while others may focus more on imaginative play such as storytelling, puppetry, and role-playing (Göncü, 1993; Leisterer-Peoples, 2021; Stengelin et al., 2020; Stengelin et al., 2023).
One culture that emphasizes physical play is that of the Maasai people in East Africa. From a young age, children are encouraged to engage in jumping contests and spear-throwing games, in addition to football (soccer), volleyball, and variations of games like tag. These activities develop physical strength and endurance and prepare children for the physical demands of a semi-nomadic lifestyle and management of natural resources and livestock (Garvey, 1990; Tian et al., 2021). In contrast, the Inuit culture in Canada and Greenland stresses imaginative play, such as storytelling and role-playing. Children are encouraged to develop their creativity, often using natural materials such as snow, ice, and animal skins to create their own toys and games. Storytelling is a central part of Inuit culture, and children are often taught traditional stories and legends through play and storytelling activities (Lutkenhaus & Thomsen, 2013).
The availability and use of outdoor play spaces varies as well. For example, in Scandinavian countries, outdoor play is a central part of early childhood education, and children are often encouraged to engage in unstructured play in natural settings (Dankiw et al., 2020; Einarsdóttir, 2011). Even in the winter in other northern climates, unstructured nature play is considered essential. Despite challenges due to a frigid climate much of the year, schools generally do not let weather impede scheduled outdoor activities. It not only benefits physical health, but research shows that children who participate in more nature activities show similar kindergarten-readiness as those who attend more academically focused preschools. Being outside also improves executive control, an important precursor to school success (Cordiano et al., 2019; Ernst et al., 2021; Zamzow & Ernst, 2020).
Friendships
In developmental research, a friend is defined as someone you enjoy being around and look forward to seeing again, and who feels the same about you. Forming friendships in early childhood is enormously beneficial. Children who have more opportunities to play with friends tend to develop cognitively in terms of perspective-taking, emotionally in terms of empathy and compassion, academically in terms of motivation and achievement, and even physically in terms of gross motor development from having more opportunities for outdoor play. By age 4, many children use the word “friend” when referring to certain children, and do so with a fair degree of stability (Hartup, 1983). However, among young children “friendship” is often based on proximity, such as they live next door, attend the same school, or it refers to whomever they just happen to be playing with at the time (Rubin, 1980). The term proximity refers to the circumstance of living, schooling, or vacationing near each other and on a similar schedule so there is time to socialize. The degree of similarity or resemblance needed for friendship varies by developmental age, but can be based on a match of physical characteristics, interests and hobbies, or emotional temperament. Children enjoy meeting people with similar physical and demographic characteristics. Thus, friend selection in early childhood is typically based on superficial similarities such as favorite color or the letter of a child’s first name.

Imaginary Companions
An intriguing occurrence in early childhood is the emergence of imaginary companions. Researchers differ in how they define what qualifies as an imaginary companion. Some studies include only invisible characters that the child refers to in conversation, or plays with for an extended period of time. Other researchers also include objects that the child personifies, such as a stuffed toy or doll, or characters the child impersonates every day. Estimates of the number of children who have imaginary companions vary greatly (from as little as 6% to as high as 65%) depending on what is included in the definition (Gleason et al., 2000). Little is known about why children create imaginary companions, and more than half of all companions have no obvious trigger in the child’s life (Masih, 1978). Imaginary companions are sometimes based on real people, characters from stories, or simply names the child has heard (Gleason, et. al., 2000). Imaginary companions often change over time. In their study, Gleason et al. (2000) found that 40% of the imaginary companions of the children they studied changed, such as developing superpowers, switching age, gender, or even dying, and 68% of the characteristics of the companion were acquired over time. This could reflect greater complexity in the child’s “creation” over time and/or a greater willingness to talk about their imaginary playmates. In addition, research suggests that contrary to the assumption that children with imaginary companions are compensating for poor social skills, several studies have found that these children are very sociable (Mauro, 1991; Singer & Singer, 1990; Gleason, 2002). However, studies have reported that children with imaginary companions are more likely to be first-borns or only-children (Masih, 1978; Gleason et al., 2000, Gleason, 2002). Although not all research has found a link between birth order and the incidence of imaginary playmates (Manosevitz et al., 1973). Moreover, some studies have found little or no difference in the presence of imaginary companions and parental divorce (Gleason et al., 2000), a number of people in the home, or the amount of time children are spending with real playmates (Masih, 1978; Gleason & Hohmann, 2006). Do children treat real friends differently? The answer appears to be not really. Young children view their relationship with their imaginary companion to be as supportive and nurturing as with their real friends. Gleason has suggested that this might suggest that children form a schema of what is a friend, and use this same schema in their interactions with both types of friends (Gleason et al., 2000; Gleason, 2002; Gleason & Hohmann, 2006).
Children and the Media

Media is more present in children’s lives than in the past. Most children’s media experts recommend that preschoolers should consume only one hour of high-quality educational programming per day and spend no time on any other type. Yet, media usage among young children has significantly evolved since the early 2000s, with digital devices and online platforms playing an increasingly prominent role in their lives. Recent data paints a more complex picture of early childhood media consumption:
Device Availability and Usage
Nearly all American households with children aged 0-18 (97%) had internet access in 2022, surpassing the average for all households (93%). Most children aged 3-17 access the internet via mobile phones (69%) and tablets (64%), with device preferences varying by age. In households with children under five: 98.6% have a television; 96.9% own a mobile phone; 54% have a laptop, and 49.5% have a tablet (NCHS, 2024).
Parental media habits significantly influence children’s screen time. Higher parental media usage and problematic internet use correlate with increased media use in children aged 0-4 (Riedl et al 20240). Co-viewing has become more common, with 73% of parents reporting that their children co-view at least half of the time they watch content (Kid Industries, 2023). Research has consistently shown that too much television or screen time adversely affects children’s behavior, health, and achievement (e.g., Gentile & Walsh, 2002; Robinson et al., 2001). Children exposed to TV by their second birthday were more likely to develop atypical sensory processing behaviors by 33 months old (Heffler et al., 2024). Screen time at age 1 is associated with higher risks of developmental delays in communication, fine motor, problem-solving, and personal and social skills by age 2 (Radesky et al., 2023). Excessive screen time (more than 2-3 hours/day) has been moderately associated with greater emotional lability and lower self-regulation in preschoolers (Ponti, 2023).
There can be negatives for media viewing. Young children are less able to focus on active, hands-on play while the television is on, and background TV can negatively affect cognitive and language development as well as be linked to attention problems later in childhood (Schmidt et al., 2008; Courage et al., 2010). Young children who spend too much time watching screens may not experience the beneficial interactions with their caregivers that help with facial recognition, language development, and social emotional intelligence. If television is being used as a babysitter and a substitute for high-quality time with caregivers, then this screen time is associated with children lagging in their cognitive and social emotional development.
There can also be benefits when media is used properly. Mobile educational games can be particularly helpful for early development because they can provide portable outlets for creativity, problem-solving, and interactions with others. Watching educational programs alongside a parent or caregiver and discussing what they see can be an especially effective way for children to comprehend new concepts, experiences, and ideas (Sanders et al., 2019). Screens can also help facilitate communication with family who live far away or to arrange playdates between friends following a move or, as recently happened, during a pandemic (Quinones & Adams, 2020). The recommendations for using screens in a healthy way, based on Ponti et al, 2019, can help in early childhood and beyond.
- Avoid screen time one hour before bedtime, and do not have screens in children’s bedrooms.
- Co-watch and be present when children are consuming media.
- Help children ask questions and think critically about what they are viewing, especially advertisements.
- Encourage screen use that allows for creative, educational interaction rather than passive viewing.
- Help children pick shows and videos that have positive messages and model age-appropriate behavior.
- Avoid using the TV for background noise.
- Encourage and maintain non-screen hobbies and interests.
Child Care Concerns (Ob 10)
About 75.7 percent of mothers of school-aged and 65.1 percent of mothers of preschool-aged children in the United States work outside the home (Bureau of Labor Statistics, 2018). Since more women have been entering the workplace, there has been a concern that families do not spend as much time with their children. This, however, is not true. Between 1981 and 1997, the amount of time that parents spent with children has increased overall (Sandberg & Hofferth, 2001). Modern numbers for this vary widely, as many parents who work outside of the home also devote significant amounts of time to childcare, to 14 hours a week, compared with 10 in 1965 (Geiger et al., 2019).

Seventy-five percent of children under age 5 are in scheduled child care programs. Others are cared for by family members, friends, or are in Head Start Programs. Older children are often in after-school programs, before school programs, or stay at home alone after school once they are older. Quality childcare programs can enhance a child’s social skills and can provide rich learning experiences. But long hours in poor quality care can have negative consequences for young children in particular. What determines the quality of child care? One consideration is the teacher/child ratio. States specify the maximum number of children that can be supervised by one teacher. In general, the younger the children, the more teachers required for a given number of children. The higher the teacher to child ratio, the more time the teacher has for involvement with the children and the less stressed the teacher may be so that the interactions can be more relaxed, stimulating and positive. The more children there are in a program, the less desirable the program as well. This is because the center may be more rigid in rules and structure to accommodate the large number of children in the facility. The physical environment should be colorful, stimulating, clean, and safe. The philosophy of the organization and the curriculum available should be child-centered, positive, and stimulating. Providers should be trained in early childhood education as well. A majority of states do not require training for their child care providers. And while formal education is not required for a person to provide a warm, loving relationship to a child, knowledge of a child’s development is useful for addressing their social, emotional, and cognitive needs in an effective way. By working toward improving the quality of childcare and increasing family-friendly workplace policies such as more flexible scheduling and perhaps childcare facilities at places of employment, we can accommodate families with smaller children and relieve parents of the stress sometimes associated with managing work and family life.
Preschool
Globally, as of 2021, 65% of children were enrolled in pre-primary education in GPE partner countries, compared to 19% in 2002 (GPE, 2023). In the U.S., 35% of 4-year-olds in the U.S. attended state-funded preschool programs, and 7% of 3-year-olds attended state-funded preschool programs (data does not include other types of preschools).
To set criteria for designation as a high-quality preschool, the National Association for the Education of Young Children (NAEYC) identifies 10 standards (NAEYC, 2024). These include:
- Positive relationships among all children and adults are promoted.
- A curriculum that supports learning and development in social, emotional, physical, language, and cognitive areas.
- Teaching approaches that are developmentally, culturally, and linguistically appropriate.
- Assessment of children’s progress to provide information on learning and development.
- The health and nutrition of children are promoted, while they are protected from illness and injury.
- Teachers possess the educational qualifications, knowledge, and commitment to promoting children’s learning.
- Collaborative relationships with families are established and maintained.
- Relationships with agencies and institutions in the children’s communities are established to support the program’s goals.
- Indoor and outdoor physical environments are safe and well-maintained.
- Leadership and management personnel are well qualified, effective, and maintain licensure status with the applicable state agency.

Parents should review preschool programs using the NAEYC criteria as a guide and template for asking questions that will assist them in choosing the best program for their child. Selecting the right preschool is also difficult because there are so many types of preschools available. Zachry (2013) identified Montessori, Waldorf, Reggio Emilia, High Scope, Parent Co-Ops, and Bank Street as types of preschool programs that focus on children learning through discovery. Teachers act as guides and create activities based on the child’s developmental level.
Head Start: For children who live in poverty, Head Start has been providing preschool education since 1965 when it was begun by President Lyndon Johnson as part of his war on poverty. It currently serves nearly one million children and annually costs approximately 7.5 billion dollars (United States Department of Health and Human Services, 2015). However, concerns about the effectiveness of Head Start have been ongoing since the program began. Armor (2015) reviewed existing research on Head Start and found there were no lasting gains, and the average child in Head Start had not learned more than children who did not receive preschool education.
A July 2015 evaluating the effectiveness of Head Start comes from the What Works Clearinghouse. The What Works Clearinghouse identifies research that provides reliable evidence of the effectiveness of programs and practices in education and is managed by the Institute of Education Services for the United States Department of Education. After reviewing 90 studies on the effectiveness of Head Start, only one study was deemed scientifically acceptable and this study showed disappointing results (Barshay, 2015). This study showed that 3- and 4-year-old children in Head Start received “potentially positive effects” on general reading achievement, but no noticeable effects on math achievement and social-emotional development. Nonexperimental designs are a significant problem in determining the effectiveness of Head Start programs because a control group is needed to show group differences that would demonstrate educational benefits. Because of ethical reasons, low-income children are usually provided with some type of preschool programming in an alternative setting. Additionally, Head Start programs are different depending on the location, and these differences include the length of the day or qualification of the teachers. Lastly, testing young children is difficult and strongly dependent on their language skills and comfort level with an evaluator (Barshay, 2015). The What Works Clearinghouse (WWC) has not released a comprehensive report on Head Start since 2015.
Recent research supports the Head Start program in its positive and significant impact on school readiness of preschool children, particularly those at the bottom of the achievement distribution and Spanish speakers (Bitler et al., 2016). While these gains do decline as children enter elementary school, other research points to gains that appear later in life (Currie, 2001; Luwig et al., 2007; Demig, 2009). The study conducted by Bitler et al. (2016) analyzed the effect of the Head Start program on child cognitive and social and emotional outcomes, using data from the Head Start Impact Study (HSIS), a longitudinal randomized control study of around 5,000 children ages three and four from 84 nationally representative communities in the U.S. where local Head Start programs were oversubscribed. The use of a randomized design enables the possibility to identify the effect of Head Start independently of other factors on child outcomes, and the longitudinal data allows for the impact of short-term and long-term gains. Head Start leads to positive and large gains in vocabulary knowledge and receptive language skills during the preschool period, particularly for children with low achievement levels and for Spanish-language speakers. While the early cognitive gains tend to diminish or “fade out” as children enter elementary school, there is evidence of benefits that appear in adolescence and young adulthood (Demig, 2009).
Childcare: To evaluate how early childcare affects children’s development, the National Institute of Child Health and Human Development (2006) conducted a longitudinal study. This study is considered the most comprehensive childcare study to date and began in 1991 when the children were one month of age. The study included an economically and ethnically diverse group of 1364 children assessed from 10 sites around the country. By design, the study involved single parents, minority backgrounds, and differing formal education levels. Childcare was defined as “any care provided on a regular basis by someone other than the child’s mother” (p. 4). A regular basis included more than 10 hours per week. Childcare arrangements included: Care from the father or another relative, care from a caregiver not related to the child in the child’s home, small group care in the caregiver’s home, and center-based care.
Overall results indicated that children cared for by their mothers did not develop differently than those who were cared for by others. Parents and family characteristics were stronger predictors of child development than childcare facilities. Specifically, greater cognitive, language and social competence were demonstrated when parents were more educated, had higher incomes, and provided emotionally supportive and cognitively enriched home environments. When comparing higher quality childcare with lower quality child care differences were noted. Higher quality care, as measured by adult-to-child ratios, group size, and caregivers’ educational and training levels, resulted in higher cognitive performance, better language comprehension, and production, and higher levels of school readiness. Lower quality care predicted more behavioral problems and poorer cognitive, language, and school readiness.
 The higher the teacher to child ratio, the more time the teacher has for involvement with the children and the less stressed the teacher may be so that the interactions can be more relaxed, stimulating and positive. The more children there are in a program, the less desirable the program as well. This is because the center may be more rigid in rules and structure to accommodate the large number of children in the facility. The physical environment should be colorful, stimulating, clean, and safe. The philosophy of the organization and the curriculum available should be child-centered, positive, and stimulating. Providers should be trained in early childhood education as well. A majority of states do not require training for their child care providers. While formal education is not required for a person to provide a warm, loving relationship to a child, knowledge of a child’s development is useful for addressing their social, emotional, and cognitive needs in an effective way.
The higher the teacher to child ratio, the more time the teacher has for involvement with the children and the less stressed the teacher may be so that the interactions can be more relaxed, stimulating and positive. The more children there are in a program, the less desirable the program as well. This is because the center may be more rigid in rules and structure to accommodate the large number of children in the facility. The physical environment should be colorful, stimulating, clean, and safe. The philosophy of the organization and the curriculum available should be child-centered, positive, and stimulating. Providers should be trained in early childhood education as well. A majority of states do not require training for their child care providers. While formal education is not required for a person to provide a warm, loving relationship to a child, knowledge of a child’s development is useful for addressing their social, emotional, and cognitive needs in an effective way.
By working toward improving the quality of childcare and increasing family-friendly workplace policies, such as more flexible scheduling and childcare facilities at places of employment, we can accommodate families with smaller children and relieve parents of the stress sometimes associated with managing work and family life.
Child Abuse
What’s the difference between child abuse and physical punishment during discipline? Physical or corporal punishment signifies noninjurious, openhanded hitting with the intention of modifying child behavior (Gershoff, 2008). The term “physical punishment” is more common in the United States while “corporal punishment” is used internationally. Parents’ goals in using corporal punishment, as in using any form of discipline, are to put an end to inappropriate or undesirable behavior and to promote positive and acceptable behavior (Gershoff, 2008). The research summarized by Gershoff indicates evidence that corporal punishment is more effective than other techniques in securing immediate child compliance. While physical punishment is better than no discipline, research reviewed indicates that physical punishment decreases moral internalization (that is, the child’s internalizing positive moral values) (Gershoff, 2010). In one meta-analysis including 27 studies, all reported studies found that the more parents used corporal punishment, the more aggressive their children were (as cited in Gershoff, 2010). Further, research from Blagg and Godfrey (2018) suggest that physical abuse can trigger an aggression mindset. Physical punishment can become abuse. In reviewing cases where Child Protective Services were called for child abuse, nearly two-thirds of the abusive incidents began as acts of physical punishment meant to correct a child’s misbehavior (Gershoff, 2010).
The Child Abuse Prevention and Treatment Act (United States Department of Health and Human Services, 2013) defines child abuse and neglect as: Any recent act or failure to act on the part of a parent or caretaker which results in death, serious physical or emotional harm, sexual abuse or exploitation; or an act or failure to act, which presents an imminent risk of serious harm (p. viii). Each state has its own definition of child abuse based on federal law, and most states recognize four major types of maltreatment: neglect, physical abuse, psychological maltreatment, and sexual abuse. Each of the forms of child maltreatment may be identified alone, but they can occur in combination.
Young children between the ages of three and six years old who are experiencing abuse or neglect are more likely to act out at daycare or preschool. They appear overly tired, strained, or worn out, and have difficulty playing with same-aged peers; they also may cry more frequently for unexplained reasons. Children who experience maltreatment are at elevated risk for emotional problems such as anxiety and depression, and behavioral problems such as ADHD, conduct problems, and aggression. Moreover, children who experience abuse and neglect are more likely to struggle academically, cognitively, and with interpersonal relationships. Over the lifespan, child abuse and neglect are related to increased prevalence of psychological disorders such as bipolar disorder, borderline personality disorder, PTSD, and substance abuse (Felitti et al, 1998; Morris & Hays-Grudo, 2023). Finally, long-term stress associated with child abuse increases the risk of inflammatory physical diseases such as heart disease, stroke, type 2 diabetes, and some cancers (Lippard et al., 2019). Broadly speaking, early childhood traumatic experiences—whether from abuse, unstable home environments, unsafe environments, or natural disasters—can increase multiple child development risks. However, early intervention and support can foster resilience in children regardless of the type of adverse experience (National Child Traumatic Stress Network, 2024; Masten & Barnes, 2018).
Victims of Child Abuse: During 2022 (the most recent year data has been collected) Child Protective Services (CPS) agencies received an estimated 4.3 million referrals involving approximately 7.5 million children (USDHHS, 2024). 89% of victims were maltreated by one or both parents. Only 3.1 millions children received prevention and post-response services. The highest rate of child abuse in children are under the age of one (22.2 per 1,000). One third to two thirds of child maltreatment cases involve substance use to some degree.
Sexual Abuse: Childhood sexual abuse is defined as any sexual contact between a child and an adult or a much older child. Incest refers to sexual contact between a child and family members. In each of these cases, the child is exploited by an older person without regard for the child’s developmental immaturity and inability to understand sexual behavior (Steele, 1986). Research estimates that 1 out of 4 girls and 1 out of 10 boys have been sexually abused (Valente, 2005). The median age for sexual abuse is 8 or 9 years for both boys and girls (Finkelhorn et al. 1990). Most boys and girls are sexually abused by a male. Although rates of sexual abuse are higher for girls than for boys, boys may be less likely to report abuse because of the cultural expectation that boys should be able to take care of themselves and because of the stigma attached to homosexual encounters (Finkelhorn et. al., 1990). Girls are more likely to be abused by a family member and boys by strangers. Sexual abuse can create feelings of self-blame, betrayal, and feelings of shame and guilt (Valente, 2005). Sexual abuse is particularly damaging when the perpetrator is someone the child trusts and may lead to depression, anxiety, problems with intimacy, and suicide (Valente, 2005).
Reporting suspected abuse: In most regions of the United States and Canada, child abuse and neglect can be reported by calling Child Protective Services (CPS). CPS is an organization that includes social workers who can meet with families and help provide resources to prevent further abuse. Services include access to counseling, anger management classes, addiction services, unemployment services, housing and shelters, and food banks. More than a third (37.5 percent) of households with children between the ages of zero and seventeen experience a visit from Child Protective Services in the United States (Kim et al., 2017). In many countries, health-care and educational professionals are required to report suspicions of abuse and neglect, but they may encounter barriers to reporting, miss signs of abuse, or feel that they lack appropriate training to confidently report concerns (Gubbels et al., 2021; Perrigo et al., 2023)
Childhood Stress and Development (Ob 13)
What is the impact of stress on child development? Not all stress is bad. Activation of our stress response systems produces a wide range of physiological reactions that prepare the body to deal with challenges or threats, including increased heart rate, elevated blood pressure, and the release of stress hormones like cortisol. When a young child has supportive caregiver relationships, these responses are brief, fostering the development of a healthy, protective stress response. Normal, everyday stress can provide an opportunity for young children to build coping skills and poses little risk to development. Even more long-lasting stressful events such as changing schools or losing a loved one can be managed fairly well. However, children who experience toxic stress or who live in extremely stressful situations of abuse over long periods of time can suffer long-lasting effects. The structures in the midbrain or limbic systems such as the hippocampus and amygdala can be vulnerable to prolonged stress during early childhood (Middlebrooks & Audage, 2008). High levels of the stress hormone cortisol can reduce the size of the hippocampus and affect the child’s memory abilities. Stress hormones can also reduce immunity to disease. The brain exposed to long periods of severe stress can develop a low threshold making the child hypersensitive to stress in the future. However, the effects of stress can be minimized if the child has the support of caring adults.
Want to learn more? Go to the Harvard’s Center for the Developing Child resources for Toxic Stress. https://developingchild.harvard.edu/key-concept/toxic-stress/
Early childhood experiences of trauma
Preschool and young school-age children exposed to a traumatic event may experience a feeling of helplessness, uncertainty about whether there is continued danger, a general fear that extends beyond the traumatic event and into other aspects of their lives, and difficulty describing in words what is bothering them or what they are experiencing emotionally (NCTSN, 2010).
This feeling of helplessness and anxiety is often expressed as a loss of previously acquired developmental skills (NCTSN, 2010). Children who experience traumatic events might not be able to fall asleep on their own or might not be able to separate from parents at school (NCTSN, 2010). Children who might have ventured out to play in the yard prior to a traumatic event now might not be willing to play in the absence of a family member (NCTSN, 2010). Often, children lose some speech and toileting skills, or their sleep is disturbed by nightmares, night terrors, or fear of going to sleep (NCTSN, 2010). In many cases, children may engage in traumatic play—a repetitive and less imaginative form of play that may represent children’s continued focus on the traumatic event or an attempt to change a negative outcome of a traumatic event (NCTSN, 2010).
Adverse Childhood Experiences (ACEs)
The toxic stress that young children endure can have a significant impact on their later lives. According to Merrick, Ford, Ports, and Guinn (2018), the foundation for lifelong health and well-being is created in childhood, as positive experiences strengthen biological systems while adverse experiences can increase mortality and morbidity. All types of abuse, neglect, and other potentially traumatic experiences that occur before the age of 18 are referred to as adverse childhood experiences (ACEs) (CDC, 2019). ACEs have been linked to risky behaviors, chronic health conditions, low life potential and early death, and as the number of ACEs increase, so does the risk for these results.
When a child experiences strong, frequent, and/or prolonged adversity without adequate adult support, the child’s stress response systems can be activated and disrupt the development of the brain and other organ systems (Harvard University, 2019). Further, ACEs can increase the risk for stress-related disease and cognitive impairment, well into the adult years. Felitti et al. (1998) found that those who had experienced four or more ACEs compared to those who had experienced none, had increased health risks for alcoholism, drug abuse, depression, suicide attempt, increase in smoking, poor self-rated health, more sexually transmitted diseases, an increase in physical inactivity and severe obesity. More ACEs showed an increased relationship to the presence of adult diseases including heart disease, cancer, chronic lung disease, skeletal fractures, and liver disease. Overall, those with multiple ACEs were likely to have multiple health risk factors later in life.
How to help: For young children, parents can offer invaluable support, by providing comfort, rest, and an opportunity to play or draw (NCTSN, 2010). Parents can be available to provide reassurance that the traumatic event is over and that the children are safe. It is helpful for parents, family, and teachers to help children verbalize their feelings so that they don’t feel alone with their emotions (NCTSN, 2010). Providing consistent caretaking by ensuring that children are picked up from school at the anticipated time and by informing children of parents’ whereabouts can provide a sense of security for children who have recently experienced a traumatic event (NCTSN, 2010). Parents, family, caregivers, and teachers may need to tolerate regression in developmental tasks for a period of time following a traumatic event (NCTSN, 2010).
Conclusion
This chapter explored the fascinating journey of early childhood, a period marked by significant advancements in physical, cognitive, and socioemotional development. We witnessed how children gain mastery over their bodies, navigate the world with burgeoning symbolic thought and language, and develop a sense of self within the context of their families and social environments.
As children progress through these formative years, they demonstrate remarkable resilience and a profound capacity for learning. By understanding the intricate interplay of developmental domains and recognizing the impact of experiences and relationships, we can better support and nurture young children as they embark on this incredible journey of discovery and growth.
Chapter Review Practice Quiz
Chapter 5 Key terms (see Glossary)
|
adverse childhood experiences (ACEs)
|
multi-tasking |
| animism | neuorplasticity |
|
athletic coach style of parenting
|
non-declarative memory
|
| authoritarian | onlooker play |
| authoritative | operational |
|
Autism Spectrum Disorder (ASD)
|
overregularization
|
|
autobiographical memory
|
parallel play |
|
clustering rehearsal
|
permissive |
| collectivistic |
physical or corporal punishment
|
| conservation |
pre-operational stage (Piaget)
|
| corpus callosum | private speech |
|
declarative memory
|
scaffolding |
| divided attention |
selective attention
|
| divided attention | self-concept |
| egocentrism | self-esteem |
|
episodic memory
|
semantic memory
|
|
executive functioning
|
sensory memory
|
| fast-mapping |
short-term or working memory
|
| fine motor skills |
social intelligence
|
|
gender constancy
|
solidarity play |
|
gender dysphoria
|
sustained attention
|
| gender identity | theory of mind |
| gender roles | toxic stress |
|
gross motor skills
|
uninvolved |
|
information-processing
|
unoccupied play |
| initiative vs guilt |
Zone of Proximal Development
|
|
long-term memory
|
Media Attributions
- Chapter_5_Early_Childhood_02 © Barney Moss is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_Include_V3_01 © Dale Crus is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_04 © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- Private: Chapter_5_Early_Childhood_Include_V3_02 © Wikimedia is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_05 © Wikimedia is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_06 © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_07 © World bank photos is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_12 © Wikipedia is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_13 © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_14 © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- Private: chapter_5_Early_Childhood_Include_V3_03
- chapter_5_Early_Childhood_Include_V3_04
- Chapter_5_Early_Childhood_15 © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_Include_V3_05 © Flickr is licensed under a CC BY (Attribution) license
- Chapter_5_Early_Childhood_16 © Lumen is licensed under a CC BY (Attribution) license
- OSX_Lifespan_05_03_VennPiaVyg
- Chapter_5_Early_Childhood_17 © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_18 © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- OSX_Lifespan_06_01_AutismSymp
- Chapter_5_Early_Childhood_19 © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_20 © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_21 © Ignite Wellington is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_22 © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_23 © Juhan Sonin is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_24 © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_25 © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_26 © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_27 © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_28 © Eden, Janine, and Jim is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_29 © Anoop Kumar is licensed under a CC BY-SA (Attribution ShareAlike) license
- 42282998222_7e7d26b35f_c is licensed under a CC BY-NC-ND (Attribution NonCommercial NoDerivatives) license
- Chapter_5_Early_Childhood_30 © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_5_Early_Childhood_Include_V3_07 © Flickr is licensed under a CC BY-SA (Attribution ShareAlike) license
the great band of commissural fibers uniting the cerebral hemispheres of higher mammals including humans
the capacity for continuous alteration of the neural pathways and synapses of the living brain and nervous system in response to experience or injury
voluntary movements with large muscle groups
voluntary movements that use smaller muscle groups for more refined or precise movement
of, relating to, or being the stage of cognitive development according to Jean Piaget’s theory in which thought is egocentric and intuitive and not yet logical or capable of performing mental tasks
refers to logical manipulation of information, so children at this stage are considered pre-operational
tendency of young children to think that everyone sees things in the same way as the child, part of pre-operational stage (Piager)
attributing lifelike qualities to objects
ability to recognize that moving or rearranging matter does not change the quantity
range of tasks a person can’t complete independently but can accomplish with support smaller zone = more independent; larger zone = needs more support
is the temporary support that parents or teachers give a child to do a task
inner speech used when engaging in tasks; may say out loud and then internalize
is the understanding that the mind can be tricked or that the mind is not always accurate
recognizing that others can think differently about situations
Autism spectrum disorder is a condition related to brain development that impacts how a person perceives and socializes with others, causing problems in social interaction and communication. The disorder also includes limited and repetitive patterns of behavior.
based on the ideas and research of several cognitive scientists studying how individuals perceive, analyze, manipulate, use, and remember information
the ability to switch our focus between tasks or external stimuli
the ability to switch our focus between tasks or external stimuli
the ability to stay on task for long periods of time
the ability to focus on a single task or stimulus while ignoring distracting information
the first stage of the memory system, and it stores sensory input in its raw form for a very brief duration; essentially long enough for the brain to register and start processing the information – Sensory Register
a memory that involves recall of information for a relatively short time (such as a few seconds) – Working Memory
a memory that involves the storage and recall of information over a long period of time (such as days, weeks, or years)
memories for facts or events that we can consciously recollect – Explicit Memories
typically automated skills that do not require conscious recollection – Implicit Memories
long-term memory of facts, information, and meanings that is not related to any specific event personally experienced in the past
long-term memory of a specific event that was personally experienced at a particular time or place in the past
our personal narrative
the group of complex mental processes and cognitive abilities (such as working memory, impulse inhibition, and reasoning) that control the skills (such as organizing tasks, remembering details, managing time, and solving problems) required for goal-directed behavior
the person rehearses previous material while adding in additional information
words are easily learned by making connections between new words and concepts already known
earn rules of grammar as they learn language but may apply these rules inappropriately at first
the mental image one has of oneself
confidence and satisfaction in oneself
Erikson stage 3, during early childhood a child will develop a sense of initiative or have a sense of guilt
a person’s internal sense of being male, female, some combination of male and female, or neither male nor female
the knowledge that gender does not change
the rights and expectations that are associated with being male or female are learned throughout childhood and into adulthood
a distressed state arising from conflict between a person’s gender identity and the sex the person has or was identified as having at birth
Parenting Style: children develop greater competence and self-confidence when parents have high, but reasonable expectations for children’s behavior, communicate well with them, are warm, loving and responsive, and use reasoning, rather than coercion as preferred responses to children’s misbehavior
Parenting Style: the traditional model of parenting in which parents make the rules and children are expected to be obedient
Parenting Style: involves holding expectations of children that are below what could be reasonably expected from them
Parenting Style: are disengaged from their children
parent style is similar to coach: Coaches and referees make sure that the rules of the game are followed and that all players adhere to those rules. Similarly, the athletic coach as a parent helps the child understand what needs to happen in certain situations whether in friendships, school, or home life and encourages and advises the child about how to manage these situations
view self as interdependent and a member of a group rather than as an independent being
children’s behavior seems more random and without a specific goal. This is the least common form of play.
Children play by themselves, do not interact with others, nor are they engaging in similar activities as the children around them.
Children are observing other children playing. They may comment on the activities and even make suggestions, but will not directly join the play
Children play alongside each other, using similar toys, but do not directly act with each other.
noninjurious, openhanded hitting with the intention of modifying child behavior
children who live in extremely stressful situations of abuse over long periods of time can suffer long-lasting effects
potentially traumatic events that occur in childhood (0-17 years)
