
Chapter 4: Infancy to Toddlerhood

Objectives:
At the end of this lesson, you will be able to…
- Summarize overall physical growth during infancy. Compare gross and fine motor skills and give examples of each.
- Describe the growth of the brain during infancy.
- Discuss nutritional concerns of marasmus and kwashiorkor.
- Describe cognitive development in infancy and toddlerhood. Describe the six substages of sensorimotor intelligence, infant memory, and language development.
- Describe stages of language development during infancy. Define babbling, holophrastic speech, and overregularization.
- Contrast styles of attachment.
- Discuss the importance of temperament and goodness of fit.
- Describe self-awareness, stranger wariness, and separation anxiety.
- Use Erikson’s theory to characterize psychosocial development during infancy.
The objectives are next to reading sections below.
Introduction
Welcome to the story of development from infancy through toddlerhood; from birth until about 2 years of age. Researchers have given this part of the life span more attention than any other period, perhaps because changes during this time are so dramatic and so noticeable and perhaps because we have assumed that what happens during these years provides a foundation for one’s life to come. However, it has been argued that the significance of development during these years has been overstated (Bruer, 1999). Nevertheless, this is a period of life that contemporary educators, healthcare providers, and parents have focused on most heavily. We will examine growth and nutrition during infancy, cognitive development during the first 2 years, and then turn our attention toward attachments formed in infancy.
Physical Development (Ob 1)
Overall Physical Growth: The average newborn in the United States weighs about 7.5 pounds and is about 20 inches in length. Average birth weight varies globally. For example, in Africa it is 6.9 pounds (3,149 grams), followed by Central America (2,874 grams or 6.33 pounds) and Asia (2,713 grams or 5.98 pounds) (Marete et al., 2020). For the first few days of life, infants typically lose about 5 percent of their body weight as they eliminate waste and get used to feeding. This often goes unnoticed by most parents but can be cause for concern for those who have a smaller infant. This weight loss is temporary, however, and is followed by a rapid period of growth. Birth weight typically doubles by five months, and the average twelve-month-old weighs 22 pounds (Graber, 2023). After the first year, growth slows, and children gain about 5 pounds in the next year. Meanwhile, infants grow about 1 inch per month during the first year, and another 4 to 5 inches by age two years (Graber, 2023) The average length at 12 months (1-year-old) typically ranges from 28.5-30.5 inches. The average length at 24 months (2-year-old) it is around 33.2-35.4 inches (CDC, 2010).
Teething occurs during the first year as well, with a first tooth typically emerging between four and six months (but sometimes after the first birthday). The bottom front teeth usually develop first, followed by the top front teeth, and most children will have all their teeth by the time they’re two or three years old.
Body Proportions: Another dramatic physical change that takes place in the first several years of life is the change in body proportions. The proportion of the head to the body is part of the reason it’s hard for a newborn (or even a two-month-old) to raise their head. The head initially makes up about 50 percent of our entire length when we are developing in the womb. At birth, the head makes up about 25 percent of our length (think about how much of your length would be head if the proportions were still the same!). By age 25 it comprises about 20 percent our length. Imagine now how difficult it must be to raise one’s head during the first year of life! And indeed, if you have ever seen a 2 to 4-month-old infant lying on the stomach trying to raise the head, you know how much of a challenge this is.

The Brain in the First Two Years (Ob 2)
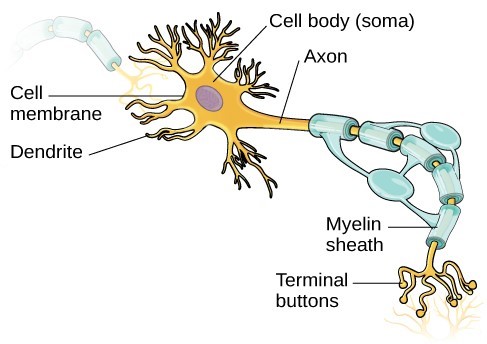
Some of the most dramatic physical change that occurs during this period is in the brain. We are born with most of the brain cells that we will ever have; that is, about 85 billion neurons whose function is to store and transmit information (Huttenlocher & Dabholkar, 1997). While most of the brain’s neurons are present at birth, they are not fully mature. During the next several years dendrites, or branching extensions that collect information from other neurons, will undergo a period of exuberance. Because of this proliferation of dendrites, by age two a single neuron might have thousands of dendrites. Synaptogenesis, or the formation of connections between neurons (connections between neurons are synapses), continues from the prenatal period forming thousands of new connections during infancy and toddlerhood. This period of rapid neural growth is referred to as Synaptic Blooming.
The blooming period of neural growth is then followed by a period of Synaptic Pruning, where neural connections are reduced thereby making those that are used much stronger. Think about how a rose bush may has become overgrown (synaptic blooming) and then it needs to be trimmed down or pruned to keep the rose bush healthy (synaptic pruning). It is thought that pruning causes the brain to function more efficiently, allowing for mastery of more complex skills (Kolb & Whishaw, 2011). Experience will shape which of these connections are maintained and which of these are lost. Ultimately, about 40 percent of these connections will be lost (Webb et al., 2001). Blooming occurs during the first few years of life, and pruning continues through childhood and into adolescence in various areas of the brain.
It is through experiences that neurons form synapses with nearby neurons, a process critical for brain development. How experiences shape the development of a child’s brain is described in this video on connections and brain development from Harvard University.
Another significant change occurring in the central nervous system is the development of Myelin, a coating of fatty tissues around the axon of the neuron (Carlson, 2014). Myelin helps to insulate the nerve cell and speed the rate of transmission of impulses from one cell to another. This enhances the building of neural pathways and improves coordination and control of movement and thought processes. The development of myelin continues into adolescence but is most dramatic during the first several years of life.
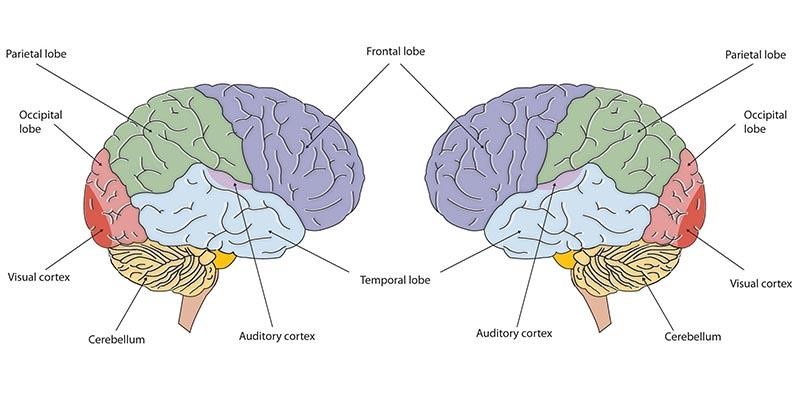
At birth, the brain is about 25 percent of its adult weight, and by age two it is at 75 percent of its adult weight. By the age of two years, a child’s brain structure typically has the appearance of an adult brain (Johnson, 2001). Most of the neural activity occurs in the cortex or the thin outer covering of the brain involved in voluntary activity and thinking. The cortex is divided into two hemispheres, and each hemisphere is divided into four lobes, each separated by folds known as fissures. If we look at the cortex starting at the front of the brain and moving over the top, we see first the frontal lobe (behind the forehead), which is responsible primarily for thinking, planning, memory, and judgment. Following the frontal lobe is the parietal lobe, which extends from the middle to the back of the skull and which is responsible primarily for processing information about touch. Next is the occipital lobe, at the very back of the skull, which processes visual information. Finally, in front of the occipital lobe, between the ears, is the temporal lobe, which is responsible for hearing and language.
Although the brain grows rapidly during infancy, specific brain regions do not mature at the same rate. Primary motor areas develop earlier than primary sensory areas, and the prefrontal cortex, which is located behind the forehead, is the least developed. As the prefrontal cortex matures, the child is increasingly able to regulate or control emotions, to plan activities, strategize, and have better judgment. This is not fully accomplished in infancy and toddlerhood but continues throughout childhood, adolescence and into adulthood.
Lateralization is the process in which different functions become localized primarily on one side of the brain. For example, in most adults, the left hemisphere is more active than the right during language production, while the reverse pattern is observed during tasks involving visuospatial abilities (Springer & Deutsch, 1993). This process develops over time. However, structural asymmetries between the hemispheres have been reported even in fetuses (Chi et al., 1997; Kasprian et al., 2011) and infants (Dubois et al., 2009). Lastly, neuroplasticity refers to the brain’s ability to change, both physically and chemically, to enhance its adaptability to environmental change, and compensate for an injury. Both environmental experiences, such as stimulation, and events within a person’s body, such as hormones and genes, affect the brain’s plasticity. So too does age. Adult brains demonstrate neuroplasticity, but they are influenced more slowly and less extensively than those of children (Kolb & Whishaw, 2011).
TRY IT!: Areas and Function of the Brain interact with the map and chart to review major areas of the brain and their functions. Toggle down on the top left menu to choose different structures to explore.
From Reflexes to Voluntary Movements (Ob 1)
If you’re having a bad day, do yourself a favor and search online for “newborn giraffes.” You’ll be greeted with funny and adorable footage of baby giraffes awkwardly standing up and trying to take their first steps mere hours after birth. What takes less than a day for a giraffe takes a year for human children, however. Why is this?
Many of our inborn motor skills are reflexes. A reflex is an involuntary movement that originates in our brainstem in response to stimulation. Reflexes are movements that occur automatically and are signals that the infant is functioning well neurologically. Reflexes are important for brain development, and most reflexes will develop into controlled motor skills, like grasping by four months and walking by twelve months. Motor and cognitive changes start with neurons, our body’s messengers, and relevant aspects of brain development.
The table below shows different movement reflexes and the age at which they disappear. Some of the more common reflexes, such as the sucking reflex (infants suck on objects that touch their lips automatically) and rooting reflex, are essential to feeding. The grasping and stepping reflexes are eventually replaced by more voluntary behaviors. Within the first few months of life, these reflexes disappear, while other (non-movement) reflexes, such as the eye-blink, swallowing, sneezing, gagging, and withdrawal reflex stay with us as they continue to serve essential functions.
| Reflex | Description | Average Age at Which Reflex Disappears |
|---|---|---|
| Stepping | Makes stepping motion when sole of feet touches hard surface | 2 months |
| Moro | Arms fling sideways with palms up as if in falling motion | 2–4 months |
| Rooting | Turns head to side, opens mouth wide, and makes sucking motions when stroked on cheek | 3–4 months |
| Palmar grasp | Grasps a finger placed in palm | 3–6 months |
| Swimming | Kicks and makes swimming motions if placed face-down in water | 4–6 months |
| Sucking | Sucks when something is in mouth | 4 months |
| Tonic neck | Assumes fencer stance when relaxed and lying face up if someone turns head to side | 6 months |
| Plantar | Curls toes in when finger is placed below them | 9–12 months |
| Babinski | Toes fan out when foot is stroked | 12 months |
| Blinking | Blinks when eyes touch something or are exposed to sudden brightness | Stays |
| Coughing | Coughs when airway is stimulated | Stays |
| Gagging | Gags when back of mouth/throat is stimulated | Stays |
| Sneezing | Sneezes when nasal passage stimulated | Stays |
Motor Development

Motor development occurs in an orderly sequence as infants move from reflexive reactions (e.g., sucking and rooting) to more advanced motor functioning. As mentioned during the prenatal section, development occurs according to the Cephalocaudal (from head to tail) and Proximodistal (from the midline outward) principles. For instance, babies first learn to hold their heads up, then to sit with assistance, then to sit unassisted, followed later by crawling, pulling up, cruising, and then walking. As motor skills develop, there are certain developmental milestones that young children should achieve. For each milestone, there is an average age, as well as a range of ages in which the milestone should be reached. An example of a developmental milestone is a baby holding up its head. Babies on average are able to hold up their head at 6 weeks old, and 90% of babies achieve this between 3 weeks and 4 months old. If a baby is not holding up his head by 4 months old, he is showing a delay. On average, most babies sit alone at 7 months old. Sitting involves both coordination and muscle strength, and 90% of babies achieve this milestone between 5 and 9 months old. If the child is displaying delays on several milestones, that is a reason for concern, and the parent or caregiver should discuss this with the child’s pediatrician. Some developmental delays can be identified and addressed through early intervention.
During the first few months of life, infants are rapidly moving from one gross motor milestone to the next. This video shows some of the motor milestones they reach during the first three months.
The development of fine motor skills during infancy allows infants to feed themselves and explore their environment. Many of these skills are learned through play.

Gross Motor Skills: These voluntary movements involve the use of large muscle groups and are typically large movements of the arms, legs, head, and torso. These skills begin to develop first. Examples include moving to bring the chin up when lying on the stomach, moving the chest up, rocking back and forth on hands and knees. But it also includes exploring an object with one’s feet as many babies do as early as 8 weeks of age if seated in a carrier or other device that frees the hips. This may be easier than reaching for an object with the hands, which requires much more practice (Berk, 2007). Sometimes an infant will try to move toward an object while crawling and surprisingly move backward because of the greater amount of strength in the arms than in the legs!
 Fine Motor Skills: Fine motor skills are more precise movements of the hands and fingers and include the ability to reach and grasp an object. Fine motor skills use smaller muscle groups in the hands, fingers, and wrist. Newborns cannot grasp objects voluntarily but do wave their arms toward objects of interest. At about 4 months of age, the infant is able to reach for an object, first with both arms and within a few weeks, with only one arm. Grasping an object involves the use of the fingers and palm, but no thumbs. Stop reading for a moment and try to grasp an object using these fingers and the palm. How does that feel? How much control do you have over the object? If it is a pen or pencil, are you able to write with it? Can you draw a picture? The answer is probably not. Use of the thumb comes at about 9 months of age when the infant is able to grasp an object using the forefinger and thumb. This ability dramatically enhances the ability to control and manipulate an object and infants take great delight in this newfound ability. They may spend hours picking up small objects from the floor and placing them in containers. By 9 months, an infant can also watch a moving object, reach for it as it approaches, and grab it. This is quite a complicated set of actions if we remember how difficult this would have been just a few months earlier.
Fine Motor Skills: Fine motor skills are more precise movements of the hands and fingers and include the ability to reach and grasp an object. Fine motor skills use smaller muscle groups in the hands, fingers, and wrist. Newborns cannot grasp objects voluntarily but do wave their arms toward objects of interest. At about 4 months of age, the infant is able to reach for an object, first with both arms and within a few weeks, with only one arm. Grasping an object involves the use of the fingers and palm, but no thumbs. Stop reading for a moment and try to grasp an object using these fingers and the palm. How does that feel? How much control do you have over the object? If it is a pen or pencil, are you able to write with it? Can you draw a picture? The answer is probably not. Use of the thumb comes at about 9 months of age when the infant is able to grasp an object using the forefinger and thumb. This ability dramatically enhances the ability to control and manipulate an object and infants take great delight in this newfound ability. They may spend hours picking up small objects from the floor and placing them in containers. By 9 months, an infant can also watch a moving object, reach for it as it approaches, and grab it. This is quite a complicated set of actions if we remember how difficult this would have been just a few months earlier.
Cultural Aspects of Motor Development
Culture-based variations in gross motor development have been documented in populations around the world (APPT, 2018). Cultural differences in daily childrearing practices can explain accelerated and delayed onset ages relative to traditionally studied populations. For example, in Africa, infants who receive massage and exercise begin sitting and walking at earlier ages than infants who do not while in Northern China, the practice of toileting infants by laying them on their backs in sandbags for most of the day delays the onset of sitting, crawling, and walking by several months (as cited in Karasik et al., 2010). In Jamaica, babies are encouraged to skip crawling and go straight to walking as crawling is seen as demeaning and walking promotes interdependence, while crawling in European or American cultural groups promotes independence in mobility (APPT, 2018). The slowest rate of motor development documented culturally is in the Ache group in Paraguay, where independence is seen and dangerous and mobility at a young age is discouraged. Thus, infants from certain cultural groups may follow unique motor development trajectories due to culture-specific caregiving practices or cultural values/beliefs. In understanding an individual child’s motor development, it is important to consider family routines, cultural values or beliefs, and what are the parent priorities (APPT, 2018).
Dynamic Systems Theory
Dynamic systems theory explains motor development as an interaction between multiple systems. According to Esther Thelen, motor skills emerge from the interplay of internal development (cognition, senses), maturation, and environment (Thelen & Smith, 2007). For example, walking requires coordinated development of balance, muscles, movement patterns, vision, and spatial awareness. Motor development depends on both biological maturation (cerebellar growth, myelination) and environmental factors. While genetic influence is evident – identical twins show more similar motor milestone timing than fraternal twins – unique experiences can lead to different motor capabilities even in identical twins (Ooki, 2006). This dynamic systems approach has expanded beyond motor development to explain other developmental domains like cognition and language across the lifespan (Spencer et al., 2011).
Sensory Development (Ob 3)
Infants were once described as being in “a blooming, buzzing confusion” by William James, an early psychologist (Shaffer, 1985). However, current research techniques have demonstrated just how developed the newborn is, especially with organized sensory and perceptual abilities.
Vision: Vision is the most poorly developed sense at birth due to the dark environment of the womb. Newborns typically cannot see further than 8 to 16 inches away from their faces, have difficulty keeping a moving object within their gaze, and can detect contrast more than color differences. If you have ever seen a newborn struggle to see, you can appreciate the cognitive efforts being made to take in visual stimulation and build those neural pathways between the eye and the brain. When you glance at a person, where do you look? Chances are you look into their eyes. If so why? It is probably because there is more information there than in other parts of the face. Newborns do not scan objects this way; instead, they tend to look at the chin another less detailed part of the face due to their limited visual system. However, by 2 or 3 months, with an advancement of the visual system, they will seek more detail when exploring an object visually and begin showing preferences for unusual images over familiar ones and for patterns over solids and faces over patterns and three-dimensional objects over flat images. Newborns have difficulty distinguishing between colors, but within a few months are able to discrimination between colors as well as do adults. Infants can also sense depth as binocular vision develops at about 2 months of age. By 6 months, the infant can perceive depth perception in pictures as well (Sen et al., 2001). Infants who have experience crawling and exploring will pay more considerable attention to visual cues of depth and modify their actions accordingly (Berk, 2007).
Hearing: The infant’s sense of hearing is very keen at birth. If you remember, this ability to hear is evidenced as soon as the 5th month of prenatal development. In fact, an infant can distinguish between very similar sounds as early as one month after birth and can distinguish between a familiar and unfamiliar voice even earlier. Some of this ability will be lost by 7 or 8 months as a child becomes familiar with the sounds of a particular language and less sensitive to sounds that are part of an unfamiliar language.
Newborns also prefer their mother’s voices over another female when speaking the same material (DeCasper & Fifer, 1980). Additionally, they will register in utero specific information heard from their mother’s voice. DeCasper and Spence (1986) tested 16 infants (average age of 55.8 hours) whose mothers had previously read to them prenatally. The mothers read several passages to their fetuses, including the first 28 paragraphs of the Cat in the Hat, beginning when they were 7 months pregnant. The fetuses had been exposed to the stories and average of 67 times or 3.5 hours. When the experimental infants were tested, the target stories (previously heard) were more reinforcing than the novel story as measured by their rate of sucking. However, for control infants, the target stories were not more reinforcing than the novel story indicating that the experimental infants had heard them before.
Touch and Pain: Touch plays a vital role in infant development from birth, triggering important reflexes and promoting parent-infant bonding. Skin-to-skin contact (“kangaroo care”) provides health benefits for newborns, while gentle touch improves outcomes in premature infants, including mood, sleep, and growth (Mehrpisheh et al., 2022; Fadlalmola et al., 2023). Additionally, touch experiences support spatial awareness, body awareness, motor development, and learning (Seidl et al., 2023).
Immediately after birth, a newborn is sensitive to touch and temperature, and is also highly sensitive to pain, responding with crying and cardiovascular responses (Balaban & Reisenauer, 2013). Newborns who are circumcised, which is the surgical removal of the foreskin of the penis, without anesthesia experience pain as demonstrated by increased blood pressure, increased heart rate, decreased oxygen in the blood, and a surge of stress hormones (United States National Library of Medicine, 2016). Typically, local pain killers are currently used during circumcision.
Taste and Smell: Studies of taste and smell demonstrate that babies respond with different facial expressions, suggesting that certain preferences are innate. Newborns can distinguish between sour, bitter, sweet, and salty flavors and show a preference for sweet flavors. Newborns also prefer the smell of their mothers. An infant only 6 days old is significantly more likely to turn toward its own mother’s breast pad than to the breast pad of another baby’s mother (Porter et al., 1992), and within hours of birth an infant also shows a preference for the face of its own mother (Bushnell, 2001; Bushnell et al., 1989).
Infants seem to be born with the ability to perceive the world in an intermodal way; that is, through stimulation from more than one sensory modality. For example, infants who sucked on a pacifier with either a smooth or textured surface preferred to look at a corresponding (smooth or textured) visual model of the pacifier. By 4 months, infants can match lip movements with speech sounds and can match other audiovisual events. Although sensory development emphasizes the afferent processes used to take in information from the environment, these sensory processes can be affected by the infant’s developing motor abilities. Reaching, crawling, and other actions allow the infant to see, touch, and organize his or her experiences in new ways.
How are Infants Tested: Habituation Procedures that measure decreased responsiveness to a stimulus after repeated presentations have increasingly been used to evaluate infants to study the development of perceptual and memory skills. Phelps (2005) describes a habituation procedure used when measuring the rate of the sucking reflex. Researchers first measure the initial baseline rate of sucking to a pacifier equipped with transducers that measure muscle contractions. Next, an auditory stimulus is presented, such as a human voice uttering a speech sound such as “da.” The rate of sucking will typically increase with the new sound but then decrease to baseline levels as “da” is repeatedly presented, showing habituation. If the sound “ma” was then presented, the rate of sucking would again increase, demonstrating that the infant can discriminate between these two stimuli.
Additionally, the speed or efficiency with which infants show habituation has been shown to predict outcomes in behaviors such as language acquisition and verbal and nonverbal intelligence. Infants who show difficulty during habituation, or habituate at slower than average rates, have been found to be at an increased risk for significant developmental delays. Infants with Down syndrome, teratogen-exposed infants, malnourished infants, and premature infants have all been studied. Researchers have found that at the age of 16 months, high-risk infants show rates of habituation comparable to newborn infants (Phelps, 2005).
Sleep
Infants need sleep but there is variation during the first few years due to changes that happen with feedings, socialization, and cultural patterns. The America Academy of Sleep recommends 12-16 hours of sleep a day for infants 4 to 12 months old (Paruthi et al., 2016). Sleep problems can be behavior related (inconsistent routines, refusal to sleep), physical (hunger or diaper change), or medical (breathing, illness). The table below notes averages for sleeping habits of birth to 24 months, although there can be variation due to culture, environmental conditions, and family customs.
Table. Sleep averages birth – 2 years old
| Age | Average Hours of Sleep in 24 hour timeframe | Naps | Night Wakings | Other Notes |
| 0-2 months | 12-18 | 3-4 | multiple (feedings) | No distinction between day/night |
| 2-6 months | 10-18* | 2-3 | 1-2 | Sleep less during day |
| 6-12 months | 10-17* | 2 | 0-1 | Night time pattern developed |
| 12-24 months | 10-15* | 1-2 | 0-1 | Night wakings decrease |
*these are averages, recommendation is 12-16 hours for 4-12 months and 11-14 hours for 1-2 years (American Academy of Pediatrics)
Bed-sharing, or co-sleeping, is a decision made based on family customs, environmental conditions, and culture. Should infants be sharing the bed with parents? Safety should be the utmost concern for co-sleeping. Colvin et al. (2014) analyzed a total of 8207 deaths from 24 states during 2004–2012 that were contained in the National Center for the Review and Prevention of Child Deaths Case Reporting System, a database of death reports from state child death review teams. The results indicated that younger victims (0-3 months) were more likely to die by bed-sharing and sleeping in an adult bed/on a person. A higher percentage of older victims (4 months to 364 days) rolled into objects in the sleep environment and changed position from side/back to prone. Carpenter et al. (2013) compared infants who died of Sudden Infant Death Syndrome (SIDS) with a matched control and found that infants younger than 3 months old who slept in bed with a parent were five times more likely to die of SIDS compared to babies who slept separately from the parents, but were still in the same room. They concluded that bed sharing, even when the parents do not smoke or take alcohol or drugs, increases the risk of SIDS. However, when combined with parental smoking and maternal alcohol consumption or drug use, risks associated with bed sharing significantly increased.
The two studies discussed above were based on American statistics. What about the rest of the world? Whiting studied 136 societies. The most prominent, he found, in 50 percent of the cultures he surveyed had one bed for mother and child and father in another bed. The other three: mother and father in the same bed, with baby in another bed; all members of the family in separate beds; all members of the family together in one bed. Co-sleeping occurs in many cultures, primarily because of a more collectivist perspective that encourages a close parent-child bond and interdependent relationship (Morelli et al., 1992). In countries where co-sleeping is common, however, parents and infants typically sleep on floor mats and other hard surfaces which minimize the suffocation that can occur with bedding and mattresses (Nelson et al., 2000).
Sudden Unexpected Infant Deaths (SUID)
Each year in the United States, there are about 3,700 Sudden Unexpected Infant Deaths (SUID). These deaths occur among infants less than 1 years old and have no immediately apparent cause (CDC, 2024). The three commonly reported types of SUID are:
- Sudden Infant Death Syndrome (SIDS): SIDS is identified when the death of a healthy infant occurs suddenly and unexpectedly, and medical and forensic investigation findings (including an autopsy) are inconclusive. SIDS is the leading cause of death in infants 1 to 12 months old, and approximately 1,500 infants died of SIDS in 2013 (CDC, 2015). Because SIDS is diagnosed when no other cause of death can be determined, possible causes of SIDS are regularly researched. One leading hypothesis suggests that infants who die from SIDS have abnormalities in the area of the brainstem responsible for regulating breathing (Weekes-Shackelford & Shackelford, 2005).
- Unknown Cause: The sudden death of an infant less than one year of age that cannot be explained because a thorough investigation was not conducted and the cause of death could not be determined.
- Accidental Suffocation and Strangulation in Bed: Reasons for accidental suffocation include: Suffocation by soft bedding, another person rolling on top of or against the infant while sleeping, an infant being wedged between two objects such as a mattress and wall, and strangulation such as when an infant’s head and neck become caught between crib railings.
The combined SUID death rate declined considerably following the release of the American Academy of Pediatrics safe sleep recommendations in 1992, which advocated that infants be placed for sleep on their backs (nonprone position).These recommendations were followed by a major Back to Sleep Campaign in 1994. However, accidental suffocation and strangulation in bed mortality rates remained unchanged until the late 1990s. In 1998 death rates from accidental suffocation and strangulation in bed started to increase, and they reached the highest rate at 33.4 deaths per 100,000 live births in 2017 (CDC, 2020).
More information about SIDS
SIDS is an exclusion diagnosis, meaning there is no lab or test to confirm SIDS. Therefore there is confusion among physicians on how to correctly apply the diagnosis of SIDS. Due to the uncertainty surrounding SIDS, some jurisdictions are not using SIDS as a cause of death at all. No specific cause has been found but there is a clear connection with SIDS between sleep environment and sleep position. The Back to Sleep campaign was designed in 1994 to encourage and educate caregivers that infants need to be put in the supine position to sleep. Supine means, sleeping on their back, facing upwards. The supine sleep position does not increase the risk of choking and aspiration. Since the start of this campaign there has been a significant drop in infants sleeping in the prone sleeping position. It is recommended that infants should be placed for sleep in the supine position for every sleep period until the infant is over the age one. Supine sleeping has been proved to be 7 times more safe than prone sleeping and 2 times more safe than laying the infant on it’s side. Side sleeping is not safe and is not recommended.
| Videos about SUID
Provides updated information about the basics of SUID and prevention methods (AboutKidsHealth, 2024).
|
The AAP (American Academy of Pediatrics) recommends a safe sleep environment can reduce all infant sleep related deaths. Some of the recommendations for a safe sleep environment include use of a firm sleep surface, room-sharing without bed-sharing, and avoidance of soft bedding and overheating. Whatever the infant sleeps in should be placed in the parents room, ideally for the first year of life, but at least for the first 6 months. Infants who are brought into the bed for feeding or comforting should be returned to their own crib when the parent is ready to return to sleep. Although the prone position is said to help the child to sleep better with no arousal, a baby that falls into a deep sleep is more at risk for SIDS. Breastfeeding is associated with a reduced risk of SIDS, physiologic sleep studies showed that breastfed infants are more easily aroused from sleep than formula fed. Infants should be placed on a firm sleep surface, covered by a fitted sheet with no other bedding or soft objects to reduce the risk of SIDS and suffocation. Keep soft objects, such as pillows, pillow-like toys, quilts, comforters, sheepskins, and loose bedding, such as blankets, away from the infant’s sleep area. Sitting devices like car seats, strollers, swings, infant carriers, and infant slings, are not recommended for routine sleep for young infants in particular. Couches and armchairs are dangerous places for infants. The amount of clothing or blankets covering an infant and the room temperature are associated with an increased risk of SIDS, avoid overheating and head coverings. An infant is also at greater risk for SIDS if the mother is smoking or drinking, during and after pregnancy.
Nurses that work in postpartum areas are in a position to correctly model and give information to caregivers about how to prevent SIDS. The American Academy of Pediatrics advise that healthcare professionals, even nurses in the nursery, are good role models and make sure caregivers know SIDS reduction recommendations and are prepared for when they are discharged. Research shows that nurses do not demonstrate complete compliance with AAP positions and do not always correctly model SIDS prevention. There was a study put in place between 2 hospitals, the main question being, “Do nurses caring for infants in the well baby postpartum nursery know and practice the AAP SIDS prevention guidelines?”(Bartlow et al., 2016) Only 30.3% of infants observed fully met the AAP guidelines, including sleep position and crib environment. The observations showed that nurses are not consistently following AAP SIDS prevention guidelines. These hospitals did not have written SIDS prevention policy. More research is needed to see if this is accurate in hospitals in other places. Changes in the hospital may be what is necessary to get practices in place, implementing written policies for SIDS prevention. SIDS is a rational fear in a number of mothers. More needs to be done about educating mothers, caretakers and everyone that is caring for an infant about safe sleeping positions.
Nutrition (Ob 4,5)
Breast milk is considered the ideal diet for newborns due to the nutrition makeup of the colostrum and subsequent breastmilk production. Colostrum is produced during pregnancy and just after birth has been described as “liquid gold” (United States Department of Health and Human Services (USDHHS, 2011). It is very rich in nutrients and antibodies. Breast milk changes by the third to fifth day after birth, becoming much thinner, but containing just the right amount of fat, sugar, water, and proteins to support overall physical and neurological development. It has the right amount of calories, fat, and protein to support overall physical and neurological development, it provides a source of iron more easily absorbed in the body than the iron found in dietary supplements, it provides resistance against many diseases, it is more easily digested by infants than is formula, and it helps babies make a transition to solid foods more easily than if bottle fed. For most babies, breast milk is also easier to digest than formula. Formula fed infants experience more diarrhea and upset stomachs. The absence of antibodies in formula often results in a higher rate of ear infections and respiratory infections. Children who are breastfed have lower rates of childhood leukemia, asthma, obesity, type 1 and 2 diabetes, and a lower risk of SIDS. For all of these reasons, it is recommended that mothers breastfeed their infants until at least 6 months of age and that breast milk be used in the diet throughout the first year (U.S. Department of Health and Human Services, 2004a in Berk, 2007). Furthermore, exclusive breastfeeding for the first six months of life is recommended in both developing and developed-country settings (Kramer & Kakuma, 2009).

There has been some research, including meta-analyses, to show that breastfeeding is connected advantages with cognitive development (Anderson et al., 1999; Binns et al., 2016; Horta et al., 2015). A meta-analysis combines the results of several studies to examine the overall effect. Low birth weight infants had the most significant benefits from breastfeeding than did normal-weight infants in a meta-analysis that 20 controlled studies (Anderson et al., 1999). Breastfeeding may provide nutrients required for rapid development of the immature brain. Breastfeeding may connect to more rapid or better development of neurological function. The meta-analysis studies also showed that a longer duration of breastfeeding was accompanied by greater differences in cognitive development between breastfed and formula-fed children. Whereas normal-weight infants showed a 2.66-point difference, low-birth-weight infants showed a 5.18-point difference in IQ compared with weight-matched, formula-fed infants (Anderson et al., 1999). These studies suggest that nutrients present in breast milk may have a significant effect on neurologic development in premature and term infants. The table below makes comparisons between breastmilk and formula.
| Human Milk | Formula |
|---|---|
| Digestion: Human milk contains balanced nutrients that are easily digested by young infants. | Timing: Formula takes longer to digest, so infants can go longer between feedings and sleep for longer durations. |
| Immunity: Human milk contains immunoglobulins that provide immunity to many diseases. | Caregiver’s diet: Caregiver doesn’t need to worry about what they are eating or drinking, including alcohol. |
| Financial cost: Human milk may be less expensive or have no cost, though pumping supplies do entail a cost. | Options: Formula comes in a range of options, such as for infants with allergies or infants needing more calories for weight gain. |
| Convenience: Human milk, when breastfed, is the correct temperature, requires no extra equipment, and can be delivered immediately when nursing parent and baby are together. | Convenience: Anyone can feed the baby, which can distribute the caregiving load. Formula, when bottle fed, can also be delivered without privacy concerns in public settings. |
| Attachment: Human milk provided by breastfeeding releases oxytocin that promotes bonding. | Attachment: Any primary caregiver can use a bottle- or chestfeeding technique with formula, which can promote bonding for all caregivers. |
| Maternal health: Breastfeeding has been associated with a reduced risk of breast and ovarian cancers. | Maternal comfort or lifestyle: Formula provides a healthy option for those who cannot or prefer not to breastfeed or provide human milk. |
Several recent studies have reported that it is not just babies that benefit from breastfeeding. Breastfeeding stimulates contractions in the uterus to help it regain its normal size, and women who breastfeed are more likely to space their pregnancies further apart. Mothers who breastfeed are at lower risk of developing breast cancer, especially among higher risk racial and ethnic groups (Islami et al., 2015; Redondo et al., 2012). Women who breastfeed have lower rates of ovarian cancer (Titus-Ernstoff et al., 2010), reduced risk for developing Type 2 diabetes (Schwarz et al., 2010; Gunderson, et al., 2015), and rheumatoid arthritis (Karlson et al., 2004).
Most mothers who breastfeed in the United States stop breastfeeding at about 6-8 weeks, often in order to return to work outside the home (USDHHS, 2011). Mothers can continue to provide breast milk to their babies by expressing and freezing the milk to be bottle fed at a later time or by being available to their infants at feeding time. However, some mothers find that after the initial encouragement they receive in the hospital to breastfeed, the outside world is less supportive of such efforts. Some workplaces support breastfeeding mothers by providing flexible schedules and welcoming infants, but many do not. And the public support of breastfeeding is sometimes lacking. Women in Canada are more likely to breastfeed than are those in the United States, and the Canadian health recommendation is for breastfeeding to continue until 2 years of age. Facilities in public places in Canada such as malls, ferries, and workplaces provide more support and comfort for the breastfeeding mother and child than found in the United States.
One early argument given to promote the practice of breastfeeding was that it promoted bonding and healthy emotional development for infants. However, this does not seem to be the case. Breastfed and bottle-fed infants adjust equally well emotionally (Ferguson & Woodward, 1999). We will discuss more about bonding and emotional development later in the chapter.
In addition to the nutritional and health benefits of breastfeeding, breast milk is free! Anyone who has priced formula recently can appreciate this added incentive to breastfeeding. Prices for a month’s worth of formula can easily range from $130-200. Prices for a year’s worth of formula and feeding supplies can cost well over $1,500 (USDHHS, 2011).
Does Breastmilk increase the babies IQ over Formula?
The main question being asked by parents is if breastfeeding increases their babies IQ. The answer to that question is that breastfeeding your child breast milk doesn’t increase the child’s IQ. A baby that is given formula to drink instead of their mothers breast milk has the same effect on the baby. Breastfeeding your child breast milk does have many benefits like, it costs zero dollars to feed your child, and breastfeeding your child helps to pass on immunity, and antibodies to various diseases and illnesses to your child. Plus, it also helps to develop the baby’s growth and cognitive development (Searing, 2016). Breastfeeding also helps the baby’s build a strong gut called microbiota and it increases the bond between mother and child (Fetter, 2017). A recent research study with 11,500 babies between whether Formula or Breast milk increased IQ, the study took place in the years 1994 to 1996. The scientist tracked the children until they were 16 year of age. In the study it made the children take 9 IQ tests throughout their lives. The study concluded that the IQ of the children that were given Formula and Breast milk had relatively the same IQ (Fetter, 2017).
Scientists started thinking that the baby’s IQ is mostly determined by the baby’s genetics, and how the mother’s education really plays a part in the development of the mental part of the child’s brain/life (Imperio, 1999). Scientists also have stated that the child’s family background or environment has more of an impact on the child’s IQ than Breast milk does (Searing, L 2016). Scientists are also stating that if the parents income is below the poverty line the child’s IQ automatically declines (Searing, 2016). So socioeconomic status in life really has more of an impact on the child’s IQ than breast milk does. And the baby’s IQ is really determined by a variety of things and not breast milk.
| Video
The following video helps to explain whether breastfeeding increases a baby’s IQ or not Katie Hinde shares insights into this complex, life-giving substance and discusses the major gaps scientific research still needs to fill so we can better understand it(TedWomen, 2016). |
Eating solids
When to Introduce More Solid Foods:
The WHO, AAP, and UNICEF recommend introducing nutritious and safe solid foods at six months of age. However, the addition of solids is considered complementary feeding, because the primary source of nutrition at this stage should still be human milk and/or formula. The time to start solid foods is based on the infant’s ability to sit up, support their head, and push up with straight elbows from a lying-down position. Solid foods should not be introduced until the infant is ready. According to The Clemson University Cooperative Extension (2014), some things to look for include the infant:
- can sit up without needing support
- can hold its head up without wobbling
- shows interest in foods others are eating
- is still hungry after being breastfed or formula fed
- is able to move foods from the front to the back of the mouth
- is able to turn away when they have had enough
For many infants who are 4 to 6 months of age, breast milk or formula can be supplemented with more solid foods. The first semi-solid foods that are introduced are iron-fortified infant cereals mixed with breast milk or formula. Typically rice, oatmeal, and barley cereals are offered as a number of infants are sensitive to more wheat-based cereals. Finger foods such as toast squares, cooked vegetable strips, or peeled soft fruit can be introduced by 10-12 months. New foods should be introduced one at a time, and the new food should be fed for a few days in a row to allow the baby time to adjust to the new food. This also allows parents time to assess if the child has a food allergy. Foods that have multiple ingredients should be avoided until parents have assessed how the child responds to each ingredient separately. Foods that are sticky (such as peanut butter or taffy), cut into large chunks (such as cheese and harder meats), and firm and round (such as hard candies, grapes, or cherry tomatoes) should be avoided as they are a choking hazard. Honey and Corn syrup should be avoided as these often contain botulism spores. In children under 12 months, this can lead to death (Clemson University Cooperative Extension, 2014).

Iron Deficiency and Anemia in the United States: About 9 million children in the United States are malnourished (Children’s Welfare, 1998). The prevalence of iron deficiency anemia in 1 to 3-year-old children seems to be increasing (Kazal, 2002). There is a link between iron deficiency anemia and diminished mental, motor, and behavioral development. Toddlers who drink too much cow’s milk may also become anemic if they are not eating other healthy foods that have iron. The calcium in milk interferes with the absorption of iron in the diet as well. Many preschools and daycare centers give toddlers a drink after they have finished their meal in order to prevent spoiling their appetites. In the second year of life, iron deficiency can be prevented by the use of a diversified diet that is rich in sources of iron and vitamin C, limiting cow’s milk consumption to less than 24 oz. per day, and providing a daily iron-fortified vitamin.
Global Considerations and Malnutrition (Ob 5)
In the 1960s, formula companies led campaigns in developing countries to encourage mothers to feed their babies on infant formula. Many mothers felt that formula would be superior to breast milk and began using formula. The use of formula can certainly be healthy under conditions in which there is adequate, clean water with which to mix the formula and adequate means to sanitize bottles and nipples. However, in many of these countries, such conditions were not available, and babies often were given diluted, contaminated formula which made them become sick with diarrhea and become dehydrated. Rates of breastfeeding declined in Peru from 90 percent to 10 percent in just 8 years (Berger, 2001). These conditions continue today, and now many hospitals prohibit the distribution of formula samples to new mothers in effort to get them to rely on breastfeeding. Many of these mothers do not understand the benefits of breastfeeding and have to be encouraged and supported to promote this practice. Breastfeeding could save the lives of millions of infants each year, according to the World Health Organization, yet fewer than 40 percent of infants are breastfed exclusively for the first 6 months of life.
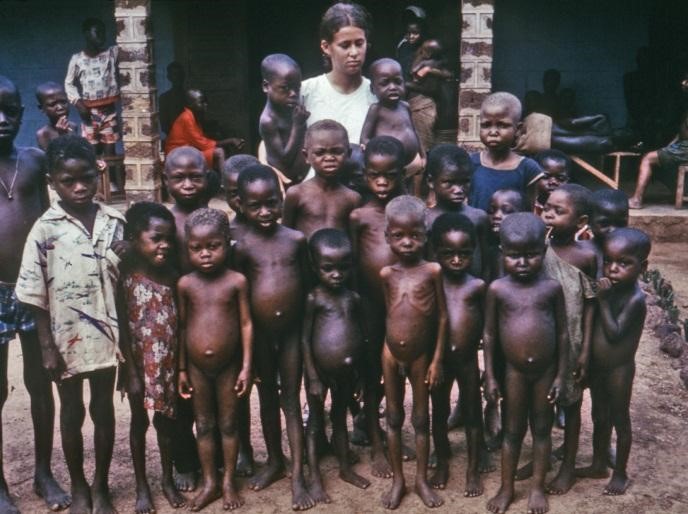
Malnutrition is responsible for 45 percent of all child deaths worldwide (WHO, 2022). Children in developing countries and countries experiencing the harsh conditions of war are at risk for two major types of malnutrition, also referred to as wasting. Infantile marasmus refers to starvation due to a lack of calories and protein. Children who do not receive adequate nutrition lose fat and muscle until their bodies can no longer function. Babies who are breastfed are much less at risk of malnutrition than those who are bottle fed. After weaning, children who have diets deficient in protein may experience kwashiorkor or the “disease of the displaced child” often occurring after another child has been born and taken over breastfeeding. This results in a loss of appetite and swelling of the abdomen as the body begins to break down the vital organs as a source of protein. Kwashiorkor can also impact a child’s cognitive development. Untreated, both marasmus and kwashiorkor can irreversibly delay physical and neurological development, leading to stunted growth, impaired cognition, and death (Alou et al., 2021; Bunker & Pandey, 2021).
Around the world, wasting continues to be a significant health crisis. According to the latest Joint Child Malnutrition Estimates, globally 45 million children under the age of 5 experience wasting, with 13.6 million suffering from severe wasting (UNICEF et al., 2023). The global prevalence stands at 6.8% of children under 5, with more than three-quarters of severely wasted children living in Asia and 22% in Africa. Economic shocks have worsened this crisis, with research showing that a 10% decline in national income can increase moderate/severe wasting prevalence by 14.4-17.8% (Osendarp et al., 2021).
The consequences of wasting depend on how late in the progression of the disease parents and guardians seek medical treatment for their children. Unfortunately, in some cultures families do not seek treatment early, and as a result by the time a child is hospitalized the child often dies within the first three days after admission (Latham, 1997). Several studies had reported long-term cognitive effects of early malnutrition (Galler & Ramsey, 1989; Galler et al., 1987; Richardson, 1980), even when home environments were controlled (Galler et al., 1990). Lower IQ scores (Galler et al., 1987), poor attention (Galler & Ramsey, 1989), and behavioral issues in the classroom (Galler et al., 1990) have been reported in children with a history of severe malnutrition in the first few years of life.
Proper nutrition is critical for optimal development during childhood, but often children in poverty have limited access to high-quality nutrition. The UNICEF website provides information about the impact of poverty on malnutrition among children across the world.
Cognitive Development (Ob 6)
Piaget and Sensorimotor Intelligence
Remember our discussion of sensorimotor development during the first two years of life from Piaget’s theory? Piaget describes intelligence in infancy as sensorimotor or based on direct, physical contact. Infants taste, feel, pound, push, hear, and move in order to experience the world. These basic motor and sensory abilities provide the foundation for the cognitive skills that will emerge during the subsequent stages of cognitive development.
How do infants connect what they are learning? Remember that Piaget believed that we are continuously trying to maintain cognitive equilibrium, or a balance, in what we see and what we know (Piaget, 1954). Children have much more of a challenge in maintaining this balance because they are continually being confronted with new situations, new words, new objects, etc. All this new information needs to be organized, and a framework for organizing information is referred to as a schema. Children develop schemata through the processes of assimilation and accommodation (review chapter 2).

We will now explore the transition infants make from responding to the external world reflexively as newborns to solving problems using mental strategies as 2-year-olds. The first stage of cognitive development is referred to as the Sensorimotor Period, and it occurs through six substages.
Substage 1: Reflexes (Birth through the 1st month). Newborns learn about their world through the use of their reflexes, such as when sucking, reaching, and grasping. This active learning begins with automatic movements or reflexes. A ball comes into contact with an infant’s cheek and is automatically sucked on and licked. Eventually, the use of these reflexes becomes more deliberate and purposeful.

Substage 2: Primary Circular Reactions (1st through the 4th month). During these next few months, the infant begins to actively involve his or her own body in some form of repeated activity. The infant begins to discriminate between objects and adjust responses accordingly as reflexes are replaced with voluntary movements. An infant may accidentally engage in a behavior and find it interesting such as making a vocalization. This interest motivates trying to do it again and helps the infant learn a new behavior that initially occurred by chance. The behavior is identified as circular and primary because it centers on the infant’s own body. At first, most actions have to do with the body, but in months to come, will be directed more toward objects.

Substage 3: Secondary Circular Reactions (4th through 8th months). The infant begins to interact with objects in the environment. At first, the infant interacts with objects (e.g., a crib mobile) accidentally, but then these contacts with the objects are deliberate and become a repeated activity. The infant becomes more and more actively engaged in the outside world and takes delight in being able to make things happen. Repeated motion brings particular interest as, for example, the infant is able to bang two lids together from the cupboard when seated on the kitchen floor.

Substage 4: Coordination of Secondary Circular Reactions (8th through 12th months). The infant combines these basic reflexes and uses planning and coordination to achieve a specific goal. Now the infant can engage in behaviors that others perform and anticipate upcoming events. Perhaps because of continued maturation of the prefrontal cortex, the infant becomes capable of having a thought and carrying out a planned, goal-directed activity. For example, an infant sees a toy car under the kitchen table and then crawls, reaches, and grabs the toy. The infant is coordinating both internal and external activities to achieve a planned goal.
Substage 5: Tertiary Circular Reactions (12th through 18th months). The toddler is considered a “little scientist” and begins exploring the world in a trial-and-error manner, using both motor skills and planning abilities. For example, the child might throw her ball down the stairs to see what happens. The toddler’s active engagement in experimentation helps them learn about their world. Gravity is learned by pouring water from a cup or pushing bowls from high chairs. The caregiver tries to help the child by picking it up again and placing it on the tray. And what happens? Another experiment! The child pushes it off the tray again causing it to fall and the caregiver to pick it up again! A closer examination of this stage causes us to really appreciate how much learning is going on at this time and how many things we come to take for granted must actually be learned. This is a wonderful and messy time of experimentation, and most learning occurs by trial and error.
 Substage 6: Beginning of Representational Thought (18th month to 2 years of age). The sensorimotor period ends with the appearance of representational (symbolic) thought. Representational (symbolic) thought is when language is linked to concepts and a child can picture of that concept in their head (mental representation). The toddler now has a basic understanding that objects can be used as symbols. Additionally, the child can solve problems using mental strategies, to remember something heard days before and repeat it, and to engage in pretend play. This initial movement from a “hands-on” approach to knowing about the world to the more mental world of sub-stage six marks the transition to preoperational thought. Take, for instance, the child who is upstairs in a room with the door closed, supposedly taking a nap. The doorknob has a safety device on it that makes it impossible for the child to turn the knob. After trying several times in vain to push the door or turn the doorknob, the child carries out a mental strategy to get the door opened-he knocks on the door! This is a technique learned from the experience of hearing a knock on the door and observing someone opening the door. The child is now better equipped with mental strategies for problem-solving. This initial movement from the “hands-on” approach to knowing about the world to the more mental world of stage six marked the transition to preoperational intelligence that we will discuss in the next lesson. Part of this stage involves learning to use language.
Substage 6: Beginning of Representational Thought (18th month to 2 years of age). The sensorimotor period ends with the appearance of representational (symbolic) thought. Representational (symbolic) thought is when language is linked to concepts and a child can picture of that concept in their head (mental representation). The toddler now has a basic understanding that objects can be used as symbols. Additionally, the child can solve problems using mental strategies, to remember something heard days before and repeat it, and to engage in pretend play. This initial movement from a “hands-on” approach to knowing about the world to the more mental world of sub-stage six marks the transition to preoperational thought. Take, for instance, the child who is upstairs in a room with the door closed, supposedly taking a nap. The doorknob has a safety device on it that makes it impossible for the child to turn the knob. After trying several times in vain to push the door or turn the doorknob, the child carries out a mental strategy to get the door opened-he knocks on the door! This is a technique learned from the experience of hearing a knock on the door and observing someone opening the door. The child is now better equipped with mental strategies for problem-solving. This initial movement from the “hands-on” approach to knowing about the world to the more mental world of stage six marked the transition to preoperational intelligence that we will discuss in the next lesson. Part of this stage involves learning to use language.
Development of Object Permanence: A critical milestone during the sensorimotor period is the development of object permanence. Object permanence is the understanding that even if something is out of sight, it still exists (Bogartz et al., 2000). Piaget thought infants do not development object permanence until 12 months, but we now know that they are capable of this milestone much earlier. Infants seem to be able to recognize that objects have permanence at much younger ages (even as young as 4 months of age). Researchers have found that even very young children understand objects and how they work long before they have experience with those objects (Baillargeon, 1987; Baillargeon et al., 2011). Infants have the beginnings of object permanence between 4 to 8 months of age. Piaget studied the acquisition of object permanence using a hide and seek toy task. He tested infants’ reactions when a toy was first shown to an infant and then hidden under a blanket. Infants who had already developed object permanence would reach for the hidden toy, indicating that they knew it still existed. Children have typically acquired object permanence by 8 months, but you will still see them make an error and reach for the wrong blanket due to limitations in memory (Johnson & Munakata, 2005). Diamond (1985) found that infants show earlier knowledge if the waiting period is shorter. At age 6 months, they retrieved the hidden object if their wait for retrieving the object is no longer than 2 seconds, and at 7 months if the wait is no longer than 4 seconds. Once toddlers have mastered object permanence, they enjoy games like hide-and-seek, and they realize that when someone leaves the room, they will come back. Toddlers also point to pictures in books and look in appropriate places when you ask them to find objects.
Piaget tested object permanence in babies by using a manual reach task with a toy and blanket. This toy and blanket method is replicated in this video, but other tasks can also assess this skill, as shown in this clip.
In Piaget’s view, around the same time children develop object permanence, they also begin to exhibit Stranger Anxiety, which is a fear of unfamiliar people (Crain, 2005). Babies may demonstrate this by crying and turning away from a stranger, by clinging to a caregiver, or by attempting to reach their arms toward familiar faces such as parents. Stranger anxiety results when a child is unable to assimilate the stranger into an existing schema; therefore, she can’t predict what her experience with that stranger will be like, which results in a fear response.
Infant Memory
Memory requires a certain degree of brain maturation, so it should not be surprising that infant memory is rather fleeting and fragile. As a result, older children and adults experience infantile amnesia, the inability to recall memories from the first few years of life. Several hypotheses have been proposed for this amnesia. From the biological perspective, it has been suggested that infantile amnesia is due to the immaturity of the infant brain, especially those areas that are crucial to the formation of autobiographical memory, such as the hippocampus. From the cognitive perspective, it has been suggested that the lack of linguistic skills of babies and toddlers limit their ability to represent events mentally; thereby, reducing their ability to encode memory. Moreover, even if infants do form such early memories, older children and adults may not be able to access them because they may be employing very different, more linguistically based, retrieval cues than infants used when forming the memory. Finally, social theorists argue that episodic memories of personal experiences may hinge on an understanding of “self,” something that is clearly lacking in infants and young toddlers.
However, in a series of clever studies Rovee-Collier and her colleagues have demonstrated that infants can remember events from their life, even if these memories are short-lived. 3-month-old infants were taught that they could make a mobile hung over their crib shake by kicking their legs. The infants were placed in their crib, on their backs. A ribbon was tied to one foot and the other end to a mobile. At first, infants made random movements, but then came to realize that by kicking they could make the mobile shake. After two 9-minute sessions with the mobile, the mobile was removed. One week later the mobile was reintroduced to one group of infants, and most of the babies immediately started kicking their legs, indicating that they remembered their prior experience with the mobile. The second group of infants was shown the mobile two weeks later, and the babies made only random movements. The memory had faded (Rovee-Collier, 1987; Giles & Rovee-Collier, 2011). Rovee-Collier and Hayne (1987) found that 3-month-olds could remember the mobile after two weeks if they were shown the mobile and watched it move, even though they were not tied to it. This reminder helped most infants to remember the connection between their kicking and the movement of the mobile. Like many researchers of infant memory, Rovee-Collier (1990) found infant memory to be very context dependent. In other words, the sessions with the mobile and the later retrieval sessions had to be conducted under very similar circumstances or else the babies would not remember their prior experiences with the mobile. For instance, if the first mobile had had yellow blocks with blue letters, but at the later retrieval session the blocks were blue with yellow letters, the babies would not kick.
Infants older than 6 months of age can retain information for more extended periods of time; they also need less reminding to retrieve information in memory. Part of their learning is attributed to joint attention, or the ability to focus on objects or individuals in social interactions. After 6 months of age, the infant’s attention becomes more social. That is, infants not only pay attention to sensations that are stimulation to them, but they also pay attention to the stimuli that seem of interest to significant others. Joint attention is important for learning the language as well as understanding emotional cues. Studies of deferred imitation, that is, the imitation of actions after a time delay, can occur as early as six months of age (Campanella & Rovee-Collier, 2005), but only if infants are allowed to practice the behavior they were shown. By 12 months of age, infants no longer need to practice the behavior in order to retain memory for four weeks (Klein & Meltzoff, 1999).

Language Development (Ob 6)
Newborn Communication
Do newborns communicate? Certainly, they do. They do not, however, communicate with the use of language. Instead, they communicate their thoughts and needs with body posture (being relaxed or still), gestures, cries, and facial expressions. A person who spends adequate time with an infant can learn which cries indicate pain and which ones indicate hunger, discomfort, or frustration.
Intentional Vocalizations: Cooing and taking turns: Infants begin to vocalize and repeat vocalizations within the first couple of months of life. That gurgling, musical vocalization called cooing can serve as a source of entertainment to an infant who has been laid down for a nap or seated in a carrier on a car ride. Cooing serves as practice for vocalization as well as the infant hears the sound of his or her own voice and tries to repeat sounds that are entertaining. Infants also begin to learn the pace and pause of conversation as they alternate their vocalization with that of someone else and then take their turn again when the other person’s vocalization has stopped. This is the start of pragmatics, the social side of language. Cooing initially involves making vowel sounds like “oooo.” Later, consonants are added to vocalizations such as “nananananana.”

Interestingly, babies replicate sounds from their own languages. A baby whose parents speak French will coo in a different tone than a baby whose parents speak Spanish or Urdu. These gurgling, musical vocalizations can serve as a source of entertainment to an infant who has been laid down for a nap or seated in a carrier on a car ride. Cooing serves as practice for vocalization, as well as the infant hears the sound of his or her own voice and tries to repeat sounds that are entertaining. Infants also begin to learn the pace and pause of conversation as they alternate their vocalization with that of someone else and then take their turn again when the other person’s vocalization has stopped.
At about 4 to six months of age, infants begin making even more elaborate vocalizations that include the sounds required for any language. Guttural sounds, clicks, consonants, and vowel sounds stand ready to equip the child with the ability to repeat whatever sounds are characteristic of the language heard. Eventually, these sounds will no longer be used as the infant grows more accustomed to a particular language.
At about 7 months, infants begin babbling, engaging in intentional vocalizations that lack specific meaning and comprise a consonant-vowel repeated sequence, such as ma-ma-ma, da-da-da. Children babble as practice in creating specific sounds, and by the time they are 1 year old, the babbling uses primarily the sounds of the language that they are learning (de Boysson-Bardies et al., 1984). These vocalizations have a conversational tone that sounds meaningful even though it is not. Babbling also helps children understand the social, communicative function of language. Children who are exposed to sign language babble in sign by making hand movements that represent real language (Petitto & Marentette, 1991).

Gesturing: Children communicate information through gesturing long before they speak, and there is some evidence that gesture usage predicts subsequent language development (Iverson & Goldin-Meadow, 2005). Deaf babies also use gestures to communicate wants, reactions, and feelings. Because gesturing seems to be easier than vocalization for some toddlers, sign language is sometimes taught to enhance one’s ability to communicate by making use of the ease of gesturing. The rhythm and pattern of language are used when deaf babies sign just as it is when hearing babies babble.
Understanding: At around ten months of age, the infant can understand more than he or she can say, which is referred to as receptive language. You may have experienced this phenomenon as well if you have ever tried to learn a second language. You may have been able to follow a conversation more easily than contribute to it. One of the first words that children understand is their own name, usually by about 6 months, followed by commonly used words like “bottle,” “mama,” and “doggie” by 10 to 12 months (Mandel et al., 1995). Infants shake their head “no” around 6–9 months, and they respond to verbal requests to do things like “wave bye-bye” or “blow a kiss” around 9–12 months. Children also use contextual information, particularly the cues that parents provide, to help them learn language. Children learn that people are usually referring to things that they are looking at when they are speaking (Baldwin, 1993), and that that the speaker’s emotional expressions are related to the content of their speech.
Holophrastic Speech: Children begin using their first words at about 12 or 13 months of age and may use partial words to convey thoughts at even younger ages. These one-word expressions are referred to as holophrastic speech. For example, the child may say “ju” for the word “juice” and use this sound when referring to a bottle. The listener must interpret the meaning of the holophrase, and when this is someone who has spent time with the child, interpretation is not too difficult. But, someone who has not been around the child will have trouble knowing what is meant. Imagine the parent who to a friend exclaims, “Ezra’s talking all the time now!” The friend hears only “ju da ga” to which the parent explains means, “I want some milk when I go with Daddy.”
Language Errors: The early utterances of children contain many errors, for instance, confusing /b/ and /d/, or /c/ and /z/. The words children create are often simplified, in part because they are not yet able to make the more complex sounds of the real language (Dobrich & Scarborough, 1992). Children may say “keekee” for kitty, “nana” for a banana, and “vesketti” for spaghetti because it is easier. Often these first words are accompanied by gestures that may also be easier to produce than the words themselves. Children’s pronunciations become increasingly accurate between 1 and 3 years, but some problems may persist until school age.
A child who learns that a word stands for an object may initially think that the word can be used for only that particular object, which is referred to as underextension. Only the family’s Irish Setter is a “doggie,” for example. More often, however, a child may think that a label applies to all objects that are similar to the original object, which is called overextension. For example, all animals become “doggies.”
First words and cultural influences: First words if the child is using English tend to be nouns. The child labels objects such as a cup, ball, or other items that they regularly interact with. In a verb-friendly language such as Chinese, however, children may learn more verbs. This may also be due to the different emphasis given to objects based on culture. Chinese children may be taught to notice action and relationships between objects, while children from the United States may be taught to name an object and its qualities (color, texture, size, etc.). These differences can be seen when comparing interpretations of art by older students from China and the United States.
Vocabulary growth spurt: 1-year-olds typically have a vocabulary of about 50 words. But by the time they become toddlers, they have a vocabulary of about 200 words and begin putting those words together in telegraphic speech (you may consider this similar to ‘text message’ speech because text messages typically only include the minimal amount of words to convey the message).
Two-word sentences and telegraphic (text message) speech: By the time they become toddlers, children have a vocabulary of about 50-200 words and begin putting those words together in telegraphic speech, such as the telephrases, “baby bye-bye” or “doggie pretty.” Words needed to convey messages are used, but the articles and other parts of speech necessary for grammatical correctness are not yet used. These expressions sound like a telegraph, or perhaps a better analogy today would be that they read like a text message. Telegraphic Speech/Text Message Speech occurs when unnecessary words are not used. “Give baby ball” is used rather than “Give the baby the ball.”

Infant-directed Speech: Why is a horse a “horsie”? Have you ever wondered why adults tend to use “baby talk” or that sing-song type of intonation and exaggeration used when talking to children? This represents a universal tendency and is known as Infant-directed Speech (child-directed speech). It involves exaggerating the vowel and consonant sounds, using a high-pitched voice, and delivering the phrase with great facial expression (Clark, 2009). Why is this done? Infants are frequently more attuned to the tone of voice of the person speaking than to the content of the words themselves and are aware of the target of speech. Werker et al. (1994) found that infants listened longer to a woman who was speaking to a baby than to a woman who was speaking to another adult. It may be in order to clearly articulate the sounds of a word so that the child can hear the sounds involved. It may also be because when this type of speech is used, the infant pays more attention to the speaker and this sets up a pattern of interaction in which the speaker and listener are in tune with one another. Interestingly, not all cultures use infant-directed speech. Research suggests that after the first few years, there are no differences in language fluency between infants who heard infant-directed speech and those raised without infant-directed speech but has a language-rich environment (Akhtar, 2005).
Baby Sign Language: A growing trend among caregivers is to use baby sign language to help infants communicate their needs before they can vocalize words. Baby sign language is a simplified form of American Sign Language with only a small subset of signs and no grammar rules. Babies start attending to signs as early as four months of age (Novack et al., 2022) and by six to eight months can learn to ask for basic needs such as milk or a diaper change. The practice can be a fun way to engage with infants, who may be less fussy if they can communicate basic needs, but research does not indicate it will enhance language and cognitive development (Kirk et al., 2013). Some in the Deaf and hard-of-hearing community have also expressed concern about hearing individuals using and modifying language intended for their community. Baby signing is not language, because it is missing the syntax, morphology, and pragmatics that make American Sign Language a full language (De Meulder, 2019). With that understanding, however, teaching babies a few signs in the first year of life may improve their ability to communicate and help parents respond to their needs (Kirk et al., 2013).
Linguistic considerations
Critical Periods: Anyone who has tried to master a second language as an adult knows the difficulty of language learning. Yet children learn languages easily and naturally. Children who are not exposed to language early in their lives will likely never learn one. Case studies, including Victor the “Wild Child,” who was abandoned as a baby in France and not discovered until he was 12, and Genie, a child whose parents kept her locked in a closet from 18 months until 13 years of age, are (fortunately) two of the only known examples of these deprived children. Both of these children made some progress in socialization after they were rescued, but neither of them ever developed language (Rymer, 1993). This is also why it is important to determine quickly if a child is deaf, and to communicate in sign language immediately. Deaf children who are not exposed to sign language during their early years will likely never learn it (Mayberry et al., 2002). The concept of critical periods highlights the importance of both nature and nurture for language development.
Social pragmatics: Language from this view is not only a cognitive skill but also a social one. Language is a tool humans use to communicate, connect to, influence, and inform others. Social pragmatics is the language and communication that individuals use during social interactions. The social nature of language has been demonstrated by a number of studies that have shown that children use several pre-linguistic skills (such as pointing, turn-taking in infancy when vocalizing, and other gestures) to communicate not only their own needs but what others may need. So, a child watching her mother search for an object may point to the object to help her mother find it.
Eighteen-month to 30-month-olds have been shown to make linguistic repairs when it is clear that another person does not understand them (Grosse et al., 2010). These researchers found that even when the child was given the desired object if there had been any misunderstanding along the way (such as a delay in being handed the object, or the experimenter calling the object by the wrong name), children would make linguistic repairs. This would suggest that children are using language not only as a means of achieving some material goal, but to make themselves understood in the mind of another person.
Brain Areas for Language: For the 90% of people who are right-handed, language is stored and controlled by the left cerebral cortex, although for some left-handers this pattern is reversed. These differences can easily be seen in the results of neuroimaging studies that show that listening to and producing language creates greater activity in the left hemisphere than in the right. Broca’s area, an area in front of the left hemisphere near the motor cortex, is responsible for language production. This area was first localized in the 1860s by the French physician Paul Broca, who studied patients with lesions to various parts of the brain. Wernicke’s area, an area of the brain next to the auditory cortex, is responsible for language comprehension.
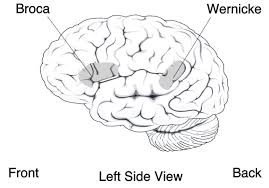
Psychosocial Development (Ob 7, 8, 9, 10)
Temperament
Perhaps you have spent time with a number of infants. How were they alike? How did they differ? How do you compare with your siblings or other children you have known well? You may have noticed that some seemed to be in a better mood than others and that some were more sensitive to noise or more easily distracted than others. These differences may be attributed to temperament. Temperament is the innate characteristics of the infant, including mood, activity level, and emotional reactivity, noticeable soon after birth. Temperamental traits are patterns of behavior that remain consistent and relatively stable throughout infancy and beyond (Goldsmith et al., 1987; Planalp & Goldsmith, 2020).
In a 1956 landmark study, Chess and Thomas (1996) evaluated 141 children’s temperament based on parental interviews. Referred to as the New York Longitudinal Study, infants were assessed on 9 dimensions of temperament including activity level, rhythmicity (regularity of biological functions), approach/withdrawal (how children deal with new things), adaptability to situations, intensity of reactions, threshold of responsiveness (how intense a stimulus has to be for the child to react), quality of mood, distractibility, attention span, and persistence.
Based on the infants’ behavioral profiles, they were categorized into three general types of temperament: Easy child, Difficult Child, and Slow to Warm Up Child
- Easy Child (40%) who is able to quickly adapt to routine and new situations, remains calm, is easy to soothe, and usually is in a positive mood.
- Difficult Child (10%) who reacts negatively to new situations, has trouble adapting to routine, is usually negative in mood, and cries frequently.
- Slow-to-Warm-Up Child (15%) has a low activity level, adjusts slowly to new situations, and is often negative in mood.
As can be seen, the percentages do not equal 100% as some children were not able to be placed neatly into one of the categories. Think about how you might approach each type of child in order to improve your interactions with them. An easy child will not need much extra attention, while a slow to warm up child may need to be given advance warning if new people or situations are going to be introduced. A difficult child may need to be given extra time to burn off their energy. A caregiver’s ability to work well and accurately read the child will enjoy a Goodness-of-Fit, meaning their styles match and communication and interaction can flow (Thomas & Chess, 1977). Parents who recognize each child’s temperament and accept it will nurture more effective interactions with the child and encourage more adaptive functioning. For example, an adventurous child whose parents regularly take her outside on hikes would provide a good “fit” to her temperament. Poorness of fit occurs when temperament is not accommodated. If a child does not adapt easily and has a low threshold, it may not be a good fit to have irregular schedules. Children are more likely to reach their potential when there is a goodness of fit. Parenting advice would be to have compatibility between the child’s dimensions of temperament and the demands and expectations in the child’s environment.
Review this video on temperamental traits to learn more about original research by Thomas and Chess.
Parenting is bidirectional: Not only do parents affect their children, but children also influence their parents. Child characteristics, such as temperament, affect parenting behaviors and roles. For example, an infant with an easy temperament may enable parents to feel more effective, as they are easily able to soothe the child and elicit smiling and cooing. On the other hand, a cranky or fussy infant elicits fewer positive reactions from his or her parents and may result in parents feeling less effective in the parenting role (Eisenberg et al., 2008). Over time, parents of more difficult children may become more punitive and less patient with their children (Clark et al., 2000; Eisenberg et al., 1999; Kiff et al., 2011). Parents who have a fussy, difficult child are less satisfied with their marriages and have greater challenges in balancing work and family roles (Hyde et al., 2004). Thus, child temperament is one of the child characteristics that influence how parents behave with their children.
Temperament does not change dramatically as we grow up, but we may learn how to work around and manage our temperamental qualities. Temperament may be one of the things about us that stays the same throughout development. In contrast, personality, defined as an individual’s consistent pattern of feeling, thinking, and behaving, is the result of the continuous interplay between biological disposition and experience. Personality also develops from temperament in other ways (Thompson et al., 2010). As children mature biologically, temperamental characteristics emerge and change over time. A newborn is not capable of much self-control, but as brain-based capacities for self-control advance, temperamental changes in self-regulation become more apparent. For example, a newborn who cries frequently doesn’t necessarily have a grumpy personality; over time, with sufficient parental support and an increased sense of security, the child might be less likely to cry. In addition, personality is made up of many other features besides temperament. Children’s developing self-concept, their motivations to achieve or to socialize, their values and goals, their coping styles, their sense of responsibility and conscientiousness, and many other qualities are encompassed into personality. These qualities are influenced by biological dispositions, but even more by the child’s experiences with others, particularly in close relationships, that guide the growth of individual characteristics. Indeed, personality development begins with the biological foundations of temperament but becomes increasingly elaborated, extended, and refined over time. The newborn that parents gazed upon thus becomes an adult with a personality of depth and nuance.
Cultural influences shape temperament differently across societies. Research has found variations in temperamental traits across countries: high activity levels in Portugal, negative mood in Lebanon, and intense mood swings in Korea (Gonda et al., 2010). These differences may reflect cultural values that encourage or discourage specific infant behaviors. For instance, U.S. adults show greater motivation for novel experiences compared to Spanish adults who are more motivated by rewards and punishment avoidance, with these differences becoming more pronounced in later childhood (Al-Halabi et al., 2011).
Infant Emotions
At birth, infants exhibit two emotional responses: Attraction and withdrawal. They show attraction to pleasant situations that bring comfort, stimulation, and pleasure, and they withdraw from unpleasant stimulation such as bitter flavors or physical discomfort. At around two months, infants exhibit social engagement in the form of social smiling as they respond with smiles to those who engage their positive attention (Lavelli & Fogel, 2005). By the end of the first year of life, infants can typically express a variety of emotions such as joy, sadness, anger, and fear. An infant may have a relatively stable and calm temperament or mood, but they can still experience a variety of emotions in a short window of time.
Social smiling becomes more stable and organized as infants learn to use their smiles to engage their parents in interactions. Pleasure is expressed as laughter at 3 to 5 months of age, and displeasure becomes more specific as fear, sadness, or anger between ages 6 and 8 months. Anger is often the reaction to being prevented from obtaining a goal, such as a toy being removed (Braungart-Rieker et al., 2010). In contrast, sadness is typically the response when infants are deprived of a caregiver (Papousek, 2007). Fear is often associated with the presence of a stranger, known as stranger wariness, or the departure of significant others known as separation anxiety. Both appear sometime between 6 and 15 months after object permanence has been acquired. Further, there is some indication that infants may experience jealousy as young as 6 months of age (Hart & Carrington, 2002).

Emotions are often divided into two general categories: Basic or primary emotions, such as interest, happiness, anger, fear, surprise, sadness, and disgust, which appear first, and self-conscious emotions, such as envy, pride, shame, guilt, doubt, and embarrassment. Unlike primary emotions, secondary emotions appear as children start to develop a self-concept, and require social instruction on when to feel such emotions. The situations in which children learn self-conscious emotions varies from culture to culture. Individualistic cultures teach us to feel pride in personal accomplishments, while in more collective cultures children are taught to not call attention to themselves unless you wish to feel embarrassed for doing so (Akimoto & Sanbinmatsu, 1999).
Facial expressions of emotion are important regulators of social interaction. In the developmental literature, this concept has been investigated under the concept of social referencing; that is, the process whereby infants seek out information from others to clarify a situation and then use that information to act (Klinnert et al., 1983). To date, the strongest demonstration of social referencing comes from work on the visual cliff. In the first study to investigate this concept, Campos and colleagues (Sorce et al., 1985) placed mothers on the far end of the “cliff” from the infant. Mothers first smiled to the infants and placed a toy on top of the safety glass to attract them; infants invariably began crawling to their mothers. When the infants were in the center of the table, however, the mother then posed an expression of fear, sadness, anger, interest, or joy. The results were clearly different for the different faces; no infant crossed the table when the mother showed fear; only 6% did when the mother posed anger, 33% crossed when the mother posed sadness, and approximately 75% of the infants crossed when the mother posed joy or interest.

Other studies provide similar support for facial expressions as regulators of social interaction. Experimenters posed facial expressions of neutral, anger, or disgust toward babies as they moved toward an object and measured the amount of inhibition the babies showed in touching the object (Bradshaw, 1986). The results for 10- and 15-month old’s were the same: Anger produced the greatest inhibition, followed by disgust, with neutral the least. This study was later replicated using joy and disgust expressions, altering the method so that the infants were not allowed to touch the toy (compared with a distractor object) until one hour after exposure to the expression (Hertenstein & Campos, 2004). At 14 months of age, significantly more infants touched the toy when they saw joyful expressions, but fewer touched the toy when the infants saw disgust.
A final emotional change is in self-regulation. Emotional self-regulation refers to strategies we use to control our emotional states so that we can attain goals (Thompson & Goodvin, 2007). This requires effortful control of emotions and initially requires assistance from caregivers (Rothbart et al., 2006). Young infants have very limited capacity to adjust their emotional states and depend on their caregivers to help soothe themselves. Caregivers can offer distractions to redirect the infant’s attention and comfort to reduce emotional distress. As areas of the infant’s prefrontal cortex continue to develop, infants can tolerate more stimulation. By 4 to 6 months, babies can begin to shift their attention away from upsetting stimuli (Rothbart et al., 2006). Older infants and toddlers can more effectively communicate their need for help and can crawl or walk toward or away from various situations (Cole et al., 2010). This aids in their ability to self-regulate. Temperament also plays a role in children’s ability to control their emotional states, and individual differences have been noted in the emotional self-regulation of infants and toddlers (Rothbart & Bates, 2006). Emotion regulation strategies for caregivers vary across cultures. Research shows U.S. families emphasize stimulating environments, Dutch families focus on structure, Italian families prioritize tactile comfort, and Korean families emphasize physical well-being and routine (Harkness et al., 2007). Cultural differences also appear in parent-infant interactions: Japanese American and European American dyads show more person-oriented interactions, while Japanese dyads demonstrate more object-oriented interactions (Bornstein et al., 2012).
Development of sense of self: Self-awareness, the realization that one is separate from others, typically emerges between 15 and 24 months of age (Kopp, 2011). This development marks an important step toward understanding social emotions such as guilt, shame, embarrassment, sympathy, and empathy. The classic mirror test by Lewis and Brooks (1978) demonstrated that before 18 months, infants view their reflection as a stranger or playmate, while after 18 months, most recognize themselves and notice marks on their face.
The timing of self-recognition development can be influenced by various factors, including maternal scaffolding, parental imitation of toddler’s behavior, and environmental experiences. While mirror self-recognition typically occurs around 18 months and photo recognition by 24 months, these milestones vary based on cultural and environmental factors. Research by Ross and colleagues (2017) found that while Scottish infants with regular mirror access performed better on mirror tests, Zambian infants without mirror access showed stronger performance on body-as-obstacle tests, demonstrating that self-awareness can develop through different pathways depending on cultural experiences.
The mirror test is a simple test used to identify the beginnings of self-recognition in infants and toddlers. Watch this video demonstrating the mirror test to learn more. Like the mirror test, the body-as-obstacle test can teach us more about infants’ and toddlers’ self-awareness. Watch this video demonstrating the body-as-obstacle test to learn more.
Self-awareness manifests in multiple ways, including body awareness, visual recognition, and language development through personal pronoun use (Courage et al., 2004). This developing sense of self enables infants to engage more fully in their world, including participation in pretend play and improved communication about their experiences (Lewis & Ramsay, 2004).

Forming Attachments
Attachment is the close bond with a caregiver from which the infant derives a sense of security. The formation of attachments in infancy has been the subject of considerable research as attachments have been viewed as foundations for future relationships. Additionally, attachments form the basis for confidence and curiosity as toddlers, and as important influences on self-concept.
Harlow’s Research: In one classic study showing if nursing was the most important factor to attachment, Wisconsin University psychologists Harry and Margaret Harlow investigated the responses of young monkeys. The infants were separated from their biological mothers, and two surrogate mothers were introduced to their cages. One, the wire mother, consisted of a round wooden head, a mesh of cold metal wires, and a bottle of milk from which the baby monkey could drink. The second mother was a foam-rubber form wrapped in a heated terry-cloth blanket. The infant monkeys went to the wire mother for food, but they overwhelmingly preferred and spent significantly more time with the warm terry-cloth mother. The warm terry-cloth mother provided no food but did provide comfort (Harlow, 1958). The infant’s need for physical closeness and touching is referred to as contact comfort. Contact comfort is believed to be the foundation for attachment. The Harlows’ studies confirmed that babies have social as well as physical needs. Both monkeys and human babies need a secure base that allows them to feel safe. From this base, they can gain the confidence they need to venture out and explore their worlds.
Bowlby’s Theory: Building on the work of Harlow and others, John Bowlby developed the concept of attachment theory. He defined attachment as the affectional bond or tie that an infant forms with the mother (Bowlby, 1969). An infant must form this bond with a primary caregiver in order to have normal social and emotional development. In addition, Bowlby proposed that this attachment bond is very powerful and continues throughout life. He used the concept of a secure base to define a healthy attachment between parent and child (Bowlby, 1982). A secure base is a parental presence that gives the child a sense of safety as the child explores the surroundings.
Bowlby said that two things are needed for a healthy attachment: The caregiver must be responsive to the child’s physical, social, and emotional needs; and the caregiver and child must engage in mutually enjoyable interactions (Bowlby, 1969). Additionally, Bowlby observed that infants would go to extraordinary lengths to prevent separation from their parents, such as crying, refusing to be comforted, and waiting for the caregiver to return. He observed that these same expressions were common to many other mammals, and consequently argued that these negative responses to separation serve an evolutionary function. Because mammalian infants cannot feed or protect themselves, they are dependent upon the care and protection of adults for survival. Thus, those infants who were able to maintain proximity to an attachment figure were more likely to survive and reproduce.

Erikson: Trust vs. Mistrust
As previously discussed in chapter 1, Erikson formulated an eight-stage theory of psychosocial development. Erikson agreed on the importance of a secure base, arguing that the most important goal of infancy was the development of a basic sense of trust in one’s caregivers. Consequently, the first stage, trust vs. mistrust, highlights the importance of attachment. Erikson maintained that the first year to year and a half of life involves the establishment of a sense of trust (Erikson, 1982). Infants are dependent and must rely on others to meet their basic physical needs as well as their needs for stimulation and comfort. A caregiver who consistently meets these needs instills a sense of trust or the belief that the world is a trustworthy place. The caregiver should not worry about overindulging a child’s need for comfort, contact, or stimulation.
Problems establishing trust: Erikson (1982) believed that mistrust could contaminate all aspects of one’s life and deprive the individual of love and fellowship with others. Consider the implications for establishing trust if a caregiver is unavailable or is upset and ill-prepared to care for a child. Or if a child is born prematurely, is unwanted, or has physical problems that make him or her less desirable to a parent. Under these circumstances, we cannot assume that the parent is going to provide the child with a feeling of trust.
Mary Ainsworth and the Strange Situation Technique
Developmental psychologist Mary Ainsworth, a student of John Bowlby, continued studying the development of attachment in infants. Ainsworth and her colleagues created a laboratory test that measured an infant’s attachment to his or her parent. The test is called The Strange Situation Technique because it is conducted in a context that is unfamiliar to the child and therefore likely to heighten the child’s need for his or her parent (Ainsworth, 1979).
During the procedure, which lasts about 20 minutes, the parent and the infant are first left alone, while the infant explores the room full of toys. Then a strange adult enters the room and talks for a minute to the parent, after which the parent leaves the room. The stranger stays with the infant for a few minutes, and then the parent again enters and the stranger leaves the room. During the entire session, a video camera records the child’s behaviors, which are later coded by trained coders. The investigators were especially interested in how the child responded to the caregiver leaving and returning to the room, referred to as the “reunion.” Based on their behaviors, the children are categorized into one of four groups where each group reflects a different kind of attachment relationship with the caregiver. One style is secure and the other three styles are referred to as insecure. Ainsworth believed these infants felt safe and secure if their caregiver was present, and she named their pattern of behavior secure attachment. A child with a secure attachment style usually explores freely while the caregiver is present and may engage with the stranger. The child will typically play with the toys and bring one to the caregiver to show and describe from time to time. The child may be upset when the caregiver departs but is also happy to see the caregiver return. Secure attachment involved the idea that the caregiver acted as a secure base for the infant; in other words, the caregiver gave the infant a safe place from which to explore the world around them (Fraley &. Spieker, 2003). Sensitive and responsive caregiving and synchrony are likely to promote secure attachment.
How common are the attachment styles among children in the United States? It is estimated that about 65 percent of children in the United States are securely attached, and 35 percent distributed among the three insecure attachment styles.
Review this video that demonstrates the Strange Situation devised by Mary Ainsworth to learn more.
Some cultural differences in attachment styles have been found (Rothbaum et al., 2010). For example, German parents value independence and Japanese mothers are typically by their children’s sides. As a result, the rate of insecure-avoidant attachments is higher in Germany and insecure-resistant attachments are higher in Japan. These differences reflect cultural variation rather than true insecurity, however (van Ijzendoorn & Sagi, 1999).
Keep in mind that methods for measuring attachment styles have been based on a model that reflects middle-class, U. S. values, and interpretation. Newer methods for assessment attachment styles involve using a Q-sort technique in which a large number of behaviors are recorded on cards and the observer sorts the cards in a way that reflects the type of behavior that occurs within the situation (Waters, 1987). There are 90 items in the third version of the Q-sort technique, and examples of the behaviors assessed include:
- When the child returns to the mother after playing, the child is sometimes fussy for no clear reason.
- When the child is upset or injured, the child will accept comforting from adults other than the mother.
- The child often hugs or cuddles against the mother, without her asking or inviting the child to do so
- When the child is upset by the mother’s leaving, the child continues to cry or even gets angry after she is gone.
At least two researchers observe the child and parent in the home for 1.5-2 hours per visit. Usually, two visits are sufficient to gather adequate information. The parent is asked if the behaviors observed are typical for the child. This information is used to test the validity of the Strange Situation classifications across age, cultures, and clinical populations.
Caregiver Interactions and the Formation of Attachment
Most developmental psychologists argue that a child has a secure attachment style when there is consistent contact from one or more caregivers who meet the physical and emotional needs of the child in a responsive and appropriate manner. In North America, this interaction may include an emotional connection in addition to adequate care. However, even in cultures where mothers do not talk, cuddle, and play with their infants, secure attachments can develop (LeVine et. al., 1994). Secure attachments can form provided the child has consistent contact and care from one or more caregivers. Consistency of contacts may be jeopardized if the infant is cared for in a daycare with a high turnover of caregivers or if institutionalized and given little more than basic physical care. And while infants who, perhaps because of being in orphanages with inadequate care, have not had the opportunity to attach in infancy can form initial secure attachments several years later, they may have more emotional problems of depression, anger, or be overly friendly as they adjust (O’Connor et al., 2003).
The insecure ambivalent style occurs when the parent is insensitive and responds inconsistently to the child’s needs. Consequently, the infant is never sure that the world is a trustworthy place or that he or she can rely on others without some anxiety. A caregiver who is unavailable, perhaps because of marital tension, substance abuse, or preoccupation with work, may send a message to the infant he or she cannot rely on having needs met. An infant who receives only sporadic attention when experiencing discomfort may not learn how to calm down. The child may cry if separated from the caregiver and also cry upon their return. They seek constant reassurance that never seems to satisfy their doubt. Keep in mind that clingy behavior can also just be part of a child’s natural disposition or temperament and does not necessarily reflect some kind of parental neglect. Additionally, a caregiver that attends to a child’s frustration can help teach them to be calm and to relax.
The insecure avoidant style is marked by insecurity, but this style is also characterized by a tendency to avoid contact with the caregiver and with others. This child may have learned that needs typically go unmet and learns that the caregiver does not provide care and cannot be relied upon for comfort, even sporadically. An insecure avoidant child learns to be more independent and disengaged.
The insecure disorganized/disoriented style represents the most insecure style of attachment and occurs when the child is given mixed, confused, and inappropriate responses from the caregiver. For example, a mother who suffers from schizophrenia may laugh when a child is hurting or cry when a child exhibits joy. The child does not learn how to interpret emotions or to connect with the unpredictable caregiver. This type of attachment is also often seen in children who have been abused. Research has shown that abuse disrupts a child’s ability to regulate their emotions (Main & Solomon, 1990).
Caregiver Consistency: Having a consistent caregiver may be jeopardized if the infant is cared for in a daycare setting with a high turnover of staff or if institutionalized and given little more than basic physical care. Infants who, perhaps because of being in orphanages with inadequate care, have not had the opportunity to attach in infancy may still form initial secure attachments several years later. However, they may have more emotional problems of depression, anger, or be overly friendly as they interact with others (O’Connor et. al., 2003).
Social Deprivation: Severe deprivation of parental attachment can lead to serious problems. According to studies of children who have not been given warm, nurturing care, they may show developmental delays, failure to thrive, and attachment disorders (Bowlby, 1982). Non-organic failure to thrive is the diagnosis for an infant who does not grow, develop, or gain weight on schedule. In addition, postpartum depression can cause even a well-intentioned mother to neglect her infant.
Reactive Attachment Disorder: Children who experience social neglect or deprivation, repeatedly change primary caregivers that limit opportunities to form stable attachments, or are reared in unusual settings (such as institutions) that limit opportunities to form stable attachments can certainly have difficulty forming attachments. According to the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (American Psychiatric Association, 2013), those children experiencing neglectful situations and also displaying markedly disturbed and developmentally inappropriate attachment behavior, such as being inhibited and withdrawn, minimal social and emotional responsiveness to others, and limited positive effect, may be diagnosed with Reactive Attachment Disorder. This disorder often occurs with developmental delays, especially in cognitive and language areas. Fortunately, the majority of severely neglected children do not develop Reactive Attachment Disorder, which occurs in less than 10% of such children. The quality of the caregiving environment after serious neglect affects the development of this disorder.
Resiliency: Being able to overcome challenges and successfully adapt is resiliency. Even young children can exhibit strong resiliency to harsh circumstances. Resiliency can be attributed to certain personality factors, such as an easy-going temperament. Some children are warm, friendly, and responsive, whereas others tend to be more irritable, less manageable, and difficult to console, and these differences play a role in attachment (Gillath et al., 2008; Seifer et al., 1996). It seems safe to say that attachment, like most other developmental processes, is affected by an interplay of genetic and socialization influences.
Receiving support from others also leads to resiliency. A positive and strong support group can help a parent and child build a strong foundation by offering assistance and positive attitudes toward the newborn and parent. In a direct test of this idea, Dutch researcher van den Boom (1994) randomly assigned some babies’ mothers to a training session in which they learned to better respond to their children’s needs. The research found that these mothers’ babies were more likely to show a secure attachment style in comparison to the mothers in a control group that did not receive training.
Erikson: Autonomy vs. Shame and Doubt
As the child begins to walk and talk, an interest in independence or autonomy replaces concern for trust. The toddler tests the limits of what can be touched, said, and explored. Erikson (1982) believed that toddlers should be allowed to explore their environment as freely as safety allows and in so doing will develop a sense of independence that will later grow to self-esteem, initiative, and overall confidence. If a caregiver is overly anxious about the toddler’s actions for fear that the child will get hurt or violate others’ expectation, the caregiver can give the child the message that he or she should be ashamed of their behavior and instill a sense of doubt in their own abilities. Parenting advice based on these ideas would be to keep your toddler safe, but let him or her learn by doing. Parenting advice would also say that shame can create a negative self-image and make them believe they are a bad person for the mistakes (“you are bad”) verses asking how they feel and explaining it was a mistake or not a good choice (“you did something bad” or “that was a bad choice”). For Erikson’s second stage, autonomy vs shame and doubt, a toddler would develop either autonomy or shame and doubt as a reflection of parenting and internalizing feedback about their behaviors.

Connecting with Infants and Toddlers: Your Impact Matters
As you study infant and toddler development, reflect on how this knowledge applies to your life and future roles as a parent, caregiver, teacher, healthcare provider, or any profession working with children:
- Personal Experiences: Think back to your own childhood. What early memories do you have? How might these experiences have shaped your development?
- Everyday Interactions: Notice infants and toddlers in your daily life – at the grocery store, park, or family gatherings. Observe their behaviors and interactions through the lens of what you’re learning.
- Brain Development: Every interaction with an infant or toddler contributes to their brain development. How does this change your perspective on the importance of early childhood?
- Cultural Influences: Reflect on how your cultural background might influence your views on child-rearing. How do these compare to other cultural practices you’re learning about?
- Technology and Development: As you use your smartphone or computer, think about how technology is shaping the environment in which today’s infants and toddlers are growing up.
Remember, the foundation for lifelong learning and well-being is built during these crucial early years. Your understanding of this stage can make a significant difference in a child’s life.
Measuring Infant Development
Psychologists have developed a number of ways to measure infant development. Some of these methods use psychophysiological measures (chapter 1) with habituation for cognitive development, while others are based on observations in standardized settings for psychosocial development (e.g., Strange Scenario from Ainsworth). A common assessment that is used to look at cognitive, motor, and behavior of infants is the Bayley Scales. The Bayley Scales of Infant and Toddler Development, Fourth Edition (Bayley-IV) comprehensively assesses children from 16 days to 42 months old (Pearson Education, 2020). Detailed information is even able to be obtained from non-verbal children. Children are evaluated in five key developmental domains, including cognition, language, social-emotional, motor, and adaptive behavior. The researcher measures the child’s performance on each task, and scores are totaled. The child’s scores are totaled and then compared to other children her/his age. By identifying developmental delays in the very young, the Bayley Scales can highlight which early intervention techniques might be most beneficial.

Conclusion
We have explored the dramatic story of the first two years of life. Rapid physical growth, neurological development, language acquisition, the movement from hands-on to mental learning, an expanding emotional repertoire, and the initial conceptions of self and others make this period of life very exciting. Over the course of the first two years, children begin to express their personalities; are mobile, can manipulate objects; and understand how certain important aspects of the world operate (e.g., object properties, schema formation). They understand the basics of how to make their wishes known, have formed attachments and relationships, and have learned basic ways of managing their emotions and impulses. In the coming chapters, we will examine how these abilities are shaped into more sophisticated mental processes, self-concepts, and social relationships during the years of early childhood.
Chapter Review Practice Quiz
Chapter 4 Key Terms (see Glossary for definitions)
| maramus | |
|
Cephalocaudal development
|
mylein |
| circumsion | neuroplasticity |
| co-sleeping |
Proximal-distal development
|
| dendrites | resiliency |
|
dynamic systems theory
|
secure attachment style
|
|
emotion self-regulation
|
self-awareness |
| fine motor skills |
social pragmatics
|
| goodness-of-fit | social smile |
|
gross motor skills
|
stranger anxiety |
|
holophrastic speech
|
Sudden Infant Death Syndrome (SIDS)
|
|
infant-directed speech
|
synaptic blooming
|
|
infantile amnesia
|
synaptic pruning |
|
Insecure ambivalent style
|
synaptogenesis |
|
Insecure avoidant style
|
temperament |
| kwashiorkor |
trust vs mistrust (Erikson theory)
|
| lateralization |
Media Attributions
- chapter_4_Infancy_To_Toddlerhood_02 © UK Department for International Development is licensed under a CC BY-SA (Attribution ShareAlike) license
- chapter_4_Infancy_To_Toddlerhood_07 © Tom Hammond is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_4_Infancy_To_Toddlerhood_08 © Lumen is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_4_Infancy_To_Toddlerhood_09 © Lumen is licensed under a CC BY-SA (Attribution ShareAlike) license
- chapter_4_Infancy_To_Toddlerhood_10 © Scott Sherrill is licensed under a CC BY-SA (Attribution ShareAlike) license
- chapter_4_Infancy_To_Toddlerhood_11 © Bemep is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_4_Infancy_To_Toddlerhood_12 © Torrey Wiley is licensed under a CC BY-ND (Attribution NoDerivatives) license
- chapter_4_Infancy_To_Toddlerhood_13 © Graham Hellewell is licensed under a CC BY-SA (Attribution ShareAlike) license
- chapter_4_Infancy_To_Toddlerhood_14 © Brent is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_4_Infancy_To_Toddlerhood_15 © Wikipedia is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_4_Infancy_To_Toddlerhood_16 © Dolanh is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_4_Infancy_To_Toddlerhood_17 is licensed under a CC BY-SA (Attribution ShareAlike) license
- chapter_4_Infancy_To_Toddlerhood_18 is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_4_Infancy_To_Toddlerhood_19 © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- Chapter_4_Infancy_To_Toddlerhood_20 © Andreas Photograph is licensed under a CC BY-SA (Attribution ShareAlike) license
- chapter_4_Infancy_To_Toddlerhood_Include_V3_03 © Wikipedia is licensed under a CC BY-SA (Attribution ShareAlike) license
- chapter_4_Infancy_To_Toddlerhood_22 © Mike Renlund is licensed under a CC BY-SA (Attribution ShareAlike) license
- chapter_4_Infancy_To_Toddlerhood_23 © Pixabay is licensed under a CC BY-SA (Attribution ShareAlike) license
- chapter_4_Infancy_To_Toddlerhood_Include_V3_04 © Flickr is licensed under a CC BY-SA (Attribution ShareAlike) license
- Private: chapter_4_Infancy_To_Toddlerhood_Include_V3_05 © Wikimedia is licensed under a CC BY-SA (Attribution ShareAlike) license
- chapter_4_Infancy_To_Toddlerhood_Include_V3_06 © Pixabay is licensed under a CC BY-ND (Attribution NoDerivatives) license
- Private: chapter_4_Infancy_To_Toddlerhood_Include_V3_07 © Wikimedia is licensed under a CC BY-SA (Attribution ShareAlike) license
- chapter_4_Infancy_To_Toddlerhood_Include_V3_08 © Flickr is licensed under a CC BY-SA (Attribution ShareAlike) license
- chapter_4_Infancy_To_Toddlerhood_Include_V3_09 © Pixabay is licensed under a CC BY (Attribution) license
- chapter_4_Infancy_To_Toddlerhood_Include_V3_10 © pxhere is licensed under a CC BY (Attribution) license
- chapter_4_Infancy_To_Toddlerhood_Include_V3_11 © Makenzie Purma is licensed under a CC BY-SA (Attribution ShareAlike) license
any of the usually branching protoplasmic processes that conduct impulses toward the body of a neuron
the formation of nerve synapses
a period of rapid neural growth
neural connections are reduced thereby making those that are used much stronger
a soft white material that forms a thick layer around the axons of some neurons and is composed chiefly of lipids (such as cerebroside and cholesterol), water, and smaller amounts of protein
the process in which different functions become localized primarily on one side of the brain
the capacity for continuous alteration of the neural pathways and synapses of the living brain and nervous system in response to experience or injury
growth during prenatal development occurs in two major directions from head to tail
growth during prenatal development occurs from the midline outward
voluntary movements with large muscle groups
voluntary movements that use smaller muscle groups for more refined or precise movement
studies the behavior of systems that exhibit internal states that evolve over time (i.e., internal dynamics) and how these systems interact with exogenously applied input, understanding development involves multiple systems and nature and nurture interact
procedure for surgical removal of the foreskin of the penis
parents and infants sleeping in close proximity to each other
the death of an apparently healthy infant usually before one year of age that is of unknown cause and occurs especially during sleep
a condition of chronic undernourishment occurring especially in children and usually caused by a diet deficient in calories and proteins
severe malnutrition in infants and children especially of impoverished regions cause by a diet low in protein
fear of unfamiliar people
inability to remember the feelings and experiences of early childhood
the ability to focus on objects or individuals in social interactions
the imitation of actions after a time delay
to make a low soft cry of a dove or a pigeon or a similar sound
producing meaningless speech sounds
expressing a complex of ideas in a single word or in a fixed phrase
unique way of talking to younger child to grab attention, uses higher pitch and sing-song cadence
language and communication rules for social interaction
innate characteristics of the infant, including mood, activity level, and emotional reactivity, noticeable soon after birth
parent style match and communication and interaction can flow - understanding child dimension of temperament
smile is with social interaction, usually develops by 6-8 weeks of age
strategies we use to control our emotional states so that we can attain goal
realization that one is separate from others, typically emerges between 15 and 24 months of age
stage 1 of Erikson theory - first year is focused on trust and responsiveness from caregiver
attachment style with responsive, consistent, appropriate manner caregiving
parent is insensitive and responds inconsistently to the child’s need
child has insecurity, characterized by a tendency to avoid contact with the caregiver and with others
insecure attachment
being able to overcome challenges and successfully adapt
Erikson second stage, toddler develops autonomy or develops shame and doubt
formal assessment for young children evaluating child’s developmental progress across multiple domains, including cognitive development, motor skills, language, social-emotional development, and adaptive behavior.
